 CLOSE SIDEBAR
CLOSE SIDEBAR
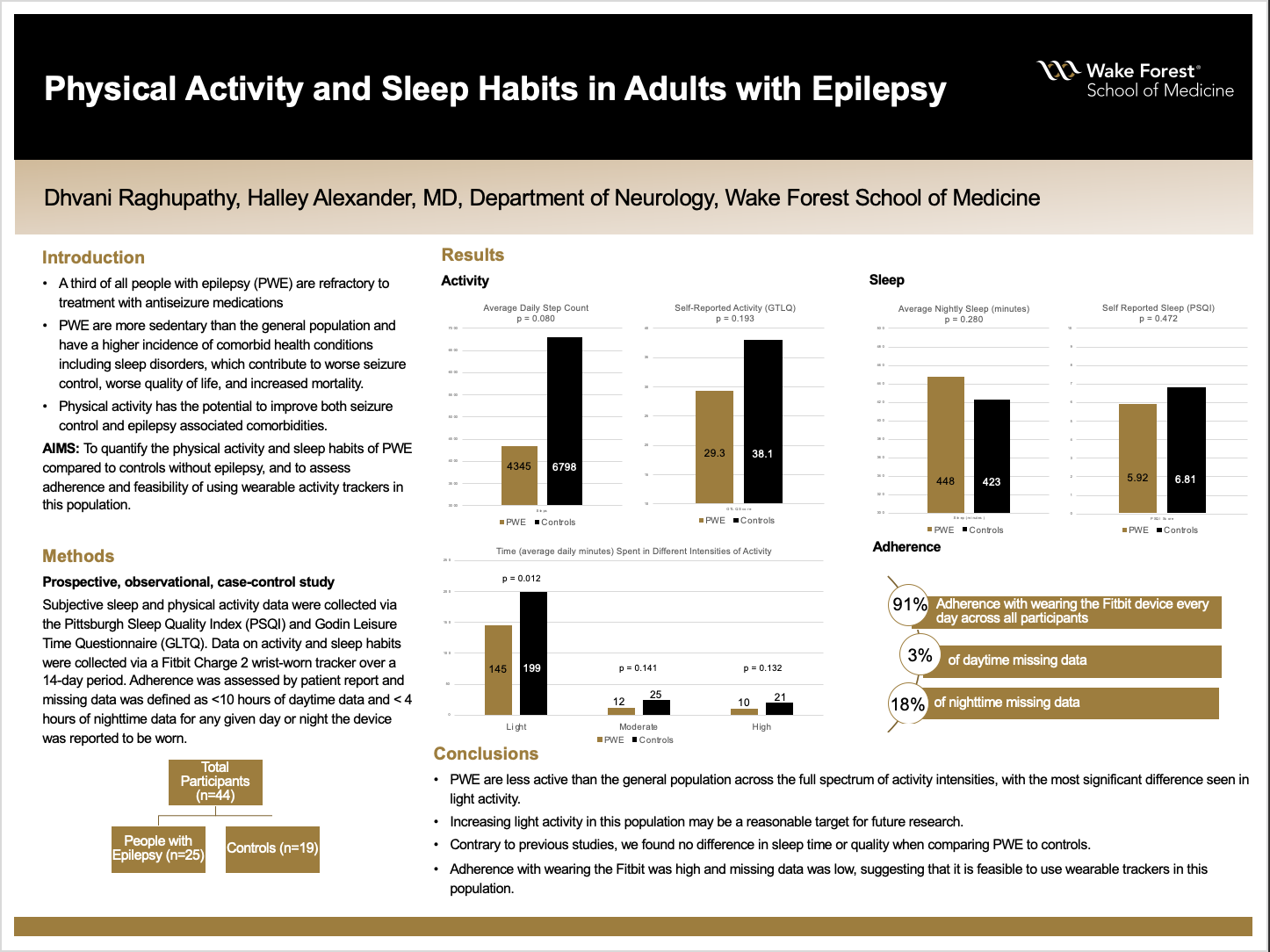
Physical Activity and Sleep Habits in Adults with Epilepsy
Dhvani Raghupathy
Background:Of the 50 million people in the world who have been diagnosed with epilepsy, about one third are refractory to treatment with antiseizure medications. There is a critical need for new therapies for epilepsy, and physical activity is a promising treatment, as animal studies have shown that physical activity may reduce seizure frequency. Moreover, people with epilepsy (PWE) have a high incidence of comorbid health conditions which include cardiovascular disease as well as sleep disorders, which contribute to worse seizure control, worse quality of life, and increased mortality in this population. Physical activity has the potential to improve both seizure control and epilepsy associated comorbidities. Prior studies have found that PWE are more sedentary compared to the general population. This study aims to quantify the physical activity and sleep habits of PWE compared to controls without epilepsy, and to assess adherence and the feasibility of data collection using wearable devices in this population.
Hypothesis:We hypothesize that 1) PWE will have a lower average daily step account, a greater amount of sedentary minutes per day, and lower self-reported activity scores compared to controls without epilepsy, 2) PWE will have a lower total sleep time in minutes per night and poorer self-reported sleep quality as measured by the Pittsburgh Sleep Quality Index (PSQI) compared to controls without epilepsy and 3) Adherence with wearing the tracker will be at or above 80% and missing data gathered from the tracker will be at or below 30%.
Methods: In this prospective, observational, case-control study, adults with focal or generalized epilepsy were recruited from the outpatient adult epilepsy clinics at the University of Virginia Health System and Wake Forest Baptist Medical Center between 2018 and 2021. At the initial visit, subjective sleep and physical activity data were collected via the Pittsburgh Sleep Quality Index (PSQI) and Godin Leisure Time Questionnaire (GLTQ). Data on activity and sleep habits were collected via a Fitbit Charge 2 wrist-worn tracker over a 14-day period. Adherence was assessed by patient report and missing data was defined as <10 hours of daytime data and < 4 hours of nighttime data for any given day or night the device was reported to be worn.
Results: A total of 44 participants completed the study. PWE had a lower average daily step counts compared to controls (4345 versus 6798, p-value 0.080) and more sedentary minutes per day (883 versus 774 minutes, p-value 0.078). When comparing time spent in light, moderate, or high intensity activity, PWE spent significantly less time in light activity per day (145 versus 199 minutes, p-value 0.012), as well as less time in moderate and high activity intensities, though these were not statistically significant. Self-reported activity levels were lower in PWE compared to controls as measured by the GLTQ (29.3 versus 38.1, p-value 0.193). Average nightly minutes of sleep (448 in PWE versus 423 in controls, p-value 0.280) and scores on the PSQI (5.92 PWE versus 6.81 controls, p-value 0.472) were similar in both groups. Adherence with wearing the Fitbit device across all participants was 91%, with 3% of daytime missing data at 18% of nighttime missing data.
Conclusions: PWE are more sedentary than the general population across the full spectrum of activity intensities, with the most significant difference seen in light activity. Focusing on increasing light activity in this population may portend benefits in seizure control and epilepsy-associated comorbidities and should be evaluated in future research. Contrary to previous studies, we found no difference in sleep time or quality when comparing PWE to controls. Adherence with wearing the Fitbit was high and missing data was low, suggesting that it is feasible to use wearable trackers in this population.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy