 CLOSE SIDEBAR
CLOSE SIDEBAR
Depressive symptoms score and risk for incident delirium: a prospective cohort study
Arlen Gaba
ABSTRACT
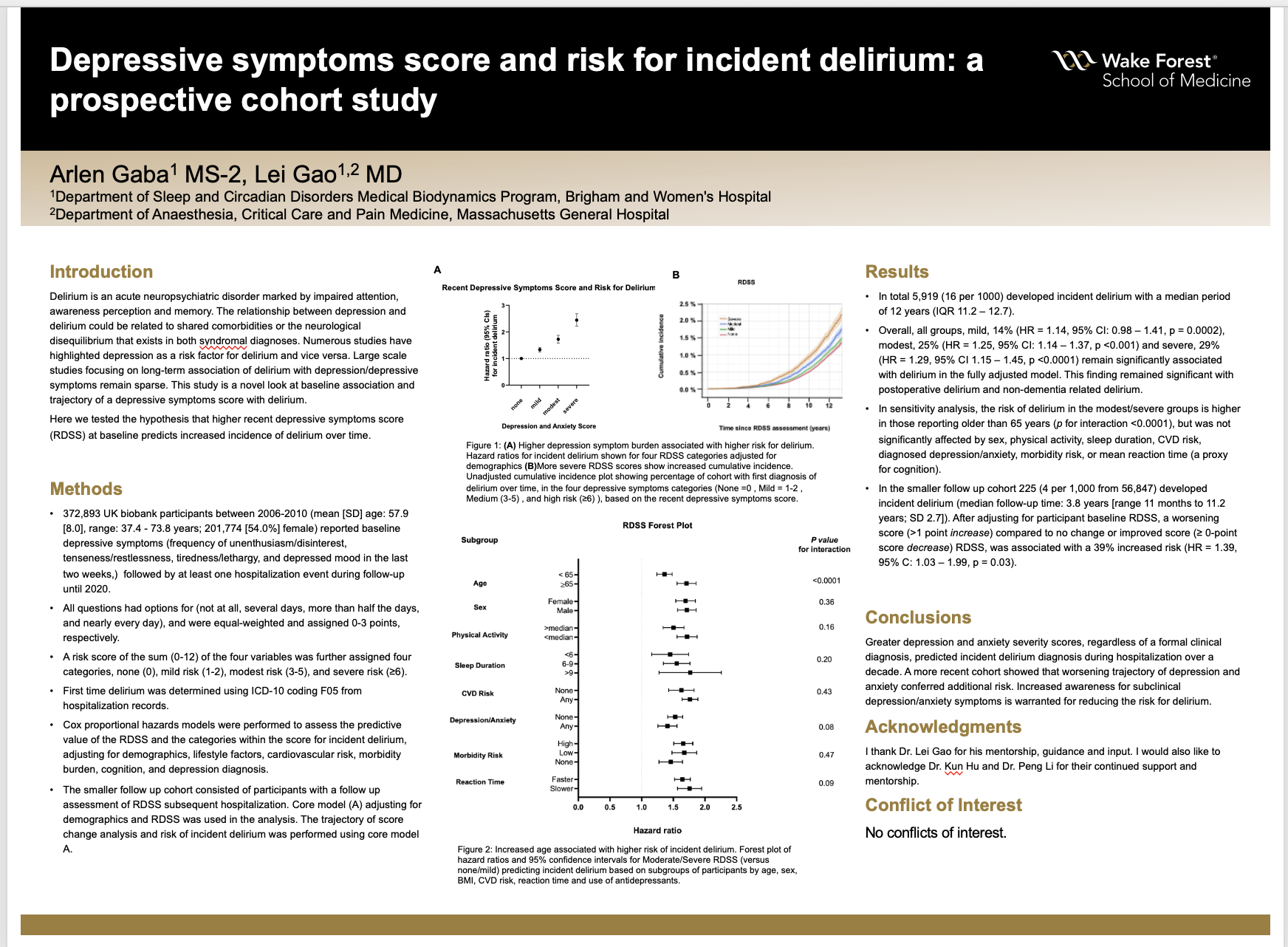
Background: Delirium is an acute neuropsychiatric disorder marked by impaired attention, awareness perception and memory. The relationship between depression and delirium could be related to shared comorbidities or the neurological disequilibrium that exists in both syndromal diagnoses. Numerous studies have highlighted depression as a risk factor for delirium and vice versa. Large scale studies focusing on long-term association of delirium with depression/depressive symptoms remain sparse. This study is a novel look at baseline association and trajectory of a depressive symptoms score with delirium.
Hypothesis: Here we tested the hypothesis that higher recent depressive symptoms score (RDSS) at baseline predicts increased incidence of delirium over time.
Methods: 372,893 UK biobank participants between 2006-2010 (mean [SD] age: 57.9 [8.0], range: 37.4 - 73.8 years; 201,774 [54.0%] female) reported baseline depressive symptoms (frequency of unenthusiasm/disinterest, tenseness/restlessness, tiredness/lethargy, and depressed mood in the last two weeks) followed by at least one hospitalization event during follow-up until 2020. All questions had options for (not at all, several days, more than half the days, and nearly every day), and were equal-weighted and assigned 0-3 points, respectively. A risk score of the sum (0-12) of the four variables was further assigned four categories, none (0), mild risk (1-2), modest risk (3-5), and severe risk (≥6). First time delirium was determined using ICD-10 coding F05 from hospitalization records. Cox proportional hazards models were performed to assess the predictive value of the RDSS and the categories within the score for incident delirium, adjusting for demographics, lifestyle factors, cardiovascular risk, morbidity burden, cognition, and depression diagnosis.
Results: In total 5,919 (16 per 1000) developed incident delirium with a median period of 12 years (IQR 11.2 – 12.7). Overall, all groups, mild, 14% (HR = 1.14, 95% CI: 0.98 – 1.41, p = 0.0002), modest, 25% (HR = 1.25, 95% CI: 1.14 – 1.37, p <0.001) and severe, 29% (HR = 1.29, 95% CI 1.15 – 1.45, p <0.0001) remain significantly associated with delirium in the fully adjusted model. This finding remained significant with postoperative delirium and non-dementia related delirium. In sensitivity analysis, the risk of delirium in the modest/severe groups is higher in those reporting older than 65 years (p for interaction <0.0001), but was not significantly affected by sex, physical activity, sleep duration, CVD risk, diagnosed depression/anxiety, morbidity risk, or mean reaction time (a proxy for cognition).
In the smaller follow up cohort 225 (4 per 1,000 from 56,847) developed incident delirium (median follow-up time: 3.8 years [range 11 months to 11.2 years; SD 2.7]). After adjusting for participant baseline RDSS, a worsening score (>1 point increase) compared to no change or improved score (≥ 0-point score decrease) RDSS, was associated with a 39% increased risk (HR = 1.39, 95% C: 1.03 – 1.99, p = 0.03).
Conclusions: Greater depression and anxiety severity scores, regardless of a formal clinical diagnosis, predicted incident delirium diagnosis during hospitalization over a decade. A more recent cohort showed that worsening trajectory of depression and anxiety conferred additional risk. Increased awareness for subclinical depression/anxiety symptoms is warranted for reducing the risk for delirium.
Source of mentor’s funding or other support that funded this research: This work was supported by NIH grant R03AG067985 and Foundations of Anesthesia and Education (FAER).
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy