 CLOSE SIDEBAR
CLOSE SIDEBAR
A Systematic Review to Assess the Domains of Disparities Affecting Outcomes in Intracerebral Hemorrhage
Priscila Arellano Zameza, M.S.
Background: Intracerebral hemorrhage (ICH) has high mortality and morbidity, with the 30-day mortality approaching 40%.1 ICH patients often need specialized care available only at tertiary care medical centers requiring interhospital transfers, and many patients expire in the first few hours of evaluation. Of the patients admitted to the WFBMC and CMC neuro ICU, 80% are admitted as interhospital transfers. These patients are at risk of delayed care, and this disproportionally affects patients from rural communities. ICH outcomes and mortality rates are not improving significantly despite several advances in stroke systems of care, and social disparities and delays in transfer account for lack of improvement outcomes.2 Multiple studies have investigated the risk factors that drive disparities in ICH and contribute to health inequity. Understanding how these drivers impact outcomes, and how providers can mitigate risk factors, is important in reducing ICH mortality and morbidity. There is heterogeneity in literature in disparities reported, outcomes evaluated, and interventions tested accounting for such inequities. There is no comprehensive resource on domains in which disparities have been identified to guide current clinical efforts and future research.
Hypothesis:We undertook a systematic review to identify and categorize all quantitative and qualitative studies on factors driving differences in ICH outcomes in the US population and define the domains in which disparities have been reported.
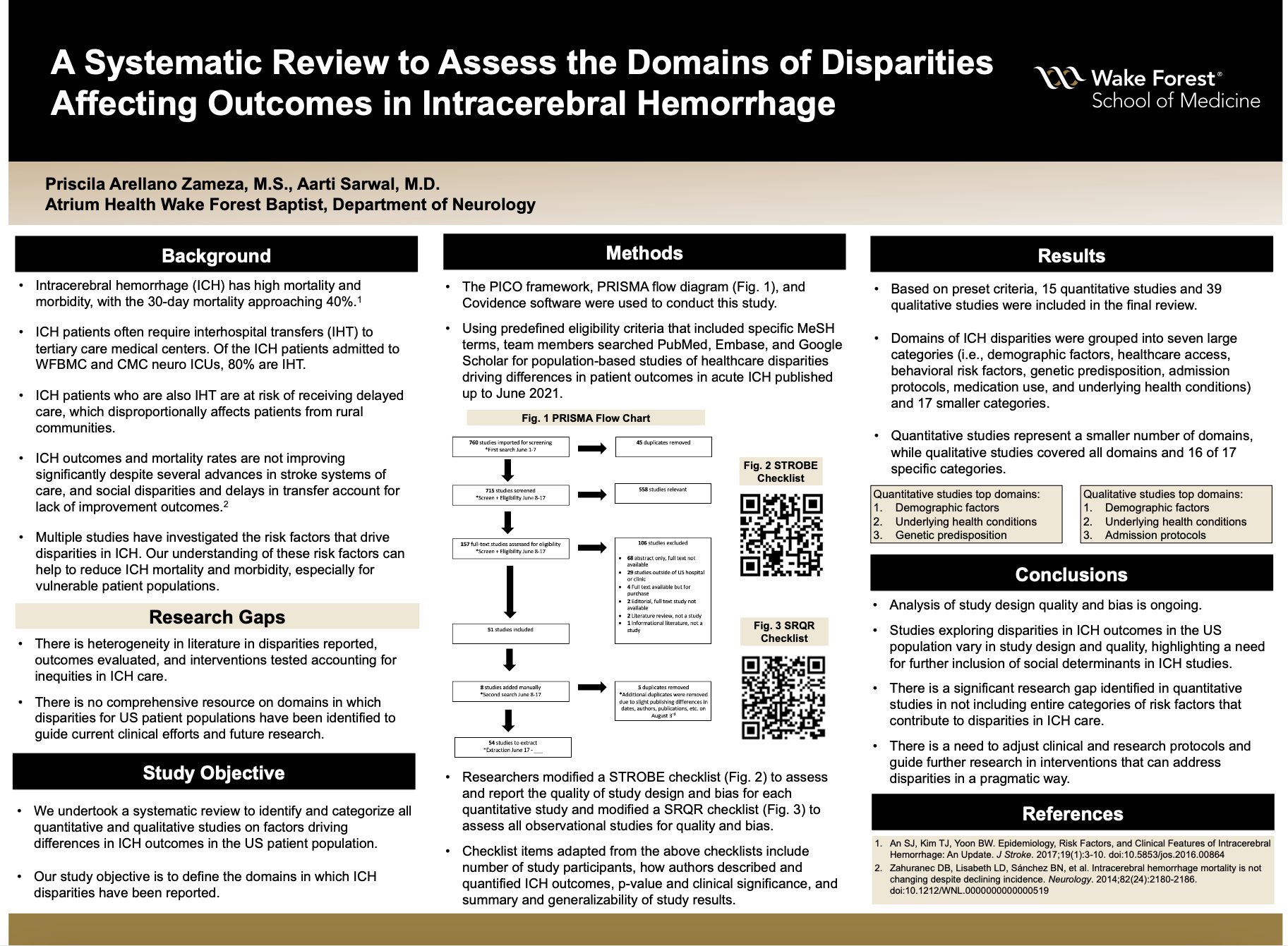
Methods:We used the PICO framework, PRISMA flow diagram, and Covidence software to conduct this systematic review. Three team members searched PubMed, Embase, and Google Scholar for population-based studies of healthcare disparities reported on acute ICH evaluation or treatment driving differences in patient outcomes using predefined eligibility criteria. Searches using a variety of MeSH terms, key terms, and filters were conducted June 2021. A modified STROBE checklist was used to assess and report the quality of study design and bias for each quantitative study, and a modified SRQR checklist to report on study design quality and bias for observational studies.
Results:A total of 760 potentially relevant studies were uploaded to Covidence. Eight additional studies were added through manual review of cited references. Based on preset criteria, 15 quantitative studies and 39 qualitative studies were included in the final review. Risk factors were grouped into seven encompassing categories. Preliminary results show that quantitative studies represent a smaller number of risk factor categories. This highlights a need for further inclusion of social determinants in ICH studies. Analysis of study design quality and bias using STROBE or SRQR checklists is ongoing.
Conclusions:Studies exploring disparities in ICH outcomes in the US population vary in study design and quality. There is a significant research gap identified in quantitative studies in not including entire categories of risk factors that contribute to disparities in ICH care. This systematic review can help healthcare professionals to account for the risk factors that impact ICH outcomes for different patient populations by adjusting clinical and research protocols. Additionally, this can help guide further research in interventions that can address disparities in a pragmatic way.
Source of mentor’s funding or other support that funded this research: None
1. An SJ, Kim TJ, Yoon BW. Epidemiology, Risk Factors, and Clinical Features of Intracerebral Hemorrhage: An Update. J Stroke. 2017;19(1):3-10. doi:10.5853/jos.2016.00864
2. Zahuranec DB, Lisabeth LD, Sánchez BN, et al. Intracerebral hemorrhage mortality is not changing despite declining incidence. Neurology. 2014;82(24):2180-2186. doi:10.1212/WNL.0000000000000519
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy