 CLOSE SIDEBAR
CLOSE SIDEBAR
Can Old Imaging Alter the Preoperative and Operative Course of Patients Undergoing Parathyroidectomy for Primary Hyperparathyroidism?
Hope Werenski
Poster Title: Can Old Imaging Alter the Preoperative and Operative Course of Patients Undergoing Parathyroidectomy for Primary Hyperparathyroidism?
Student: Hope Werenski, Class of 2023
Faculty Mentor and Department: Reese Randle, MD, General Surgery
Funding Source: None
ABSTRACT
Background:Surgical intervention provides the only definitive treatment for primary hyperparathyroidism (PHPT). Although imaging plays no role in diagnosis, it is essential for preoperative localization when a focused parathyroidectomy is planned.
Hypothesis:We hypothesized that identification of enlarged parathyroid glands on imaging obtained prior to the diagnosis of PHPT has the ability to impact the preoperative evaluation and intraoperative course of patients undergoing parathyroidectomy.
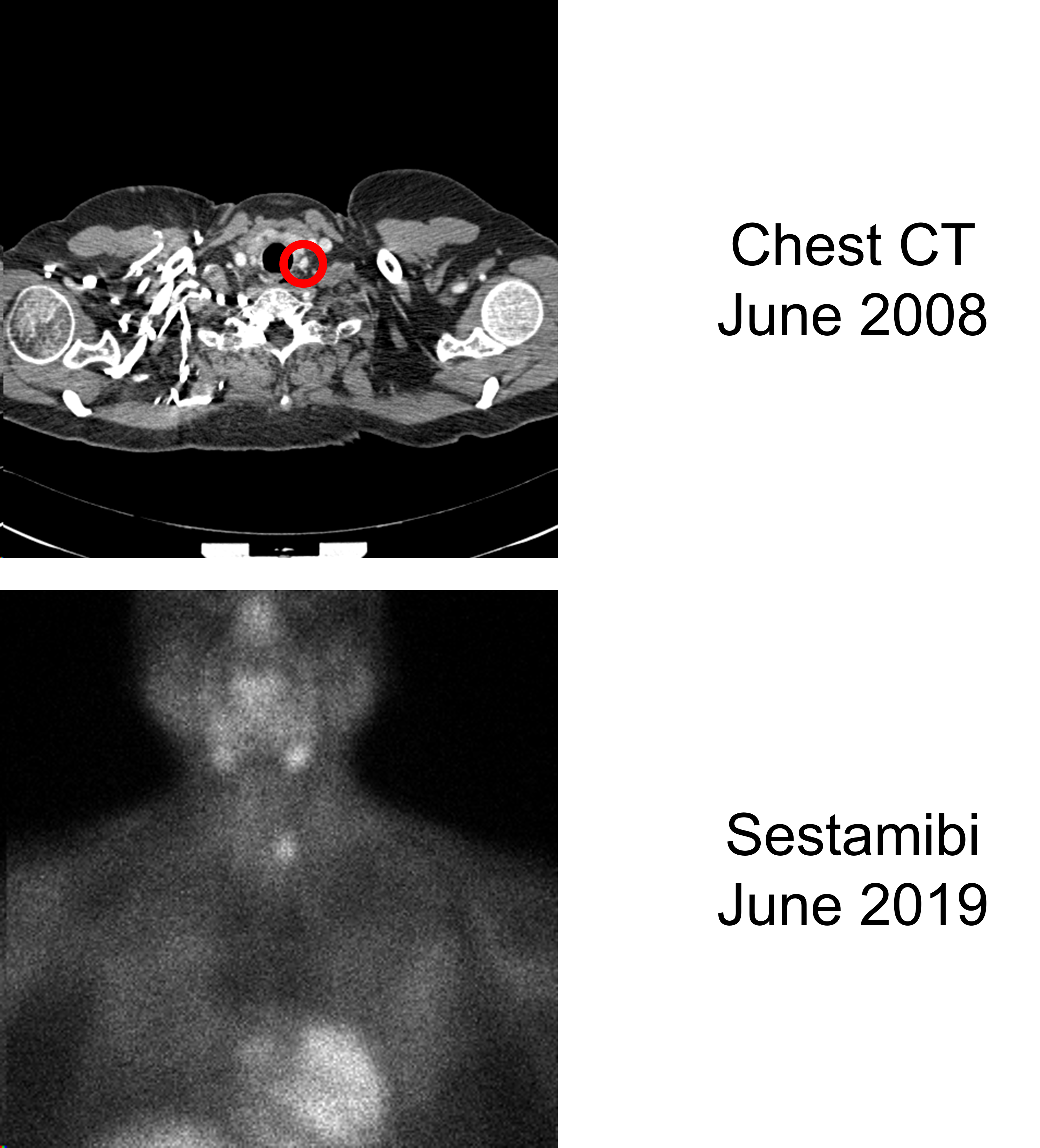
Methods:The study included adult patients with a diagnosis of PHPT who underwent parathyroidectomy between 10/2015 and 10/2020 and had contrast-enhanced CT imaging of the lower neck and upper chest prior to diagnosis for unrelated indications. A neuroradiologist retrospectively viewed these prior scans blinded to the operative findings, and a surgeon compared the imaging findings to preoperative notes and operative reports to determine whether and how information derived from prior imaging might have impacted the preoperative work-up and intraoperative course of these patients.
Results:We identified at least one visibly enlarged parathyroid gland on a prior contrast-enhanced CT in 30 (75%) of 40 included patients. The average time between the oldest scan where an enlarged parathyroid was visible and parathyroidectomy was 4.6 years (range 0.9 to 11.4). Despite old imaging enabling correct localization, 16 of these 30 (53.3%) underwent a sestamibi scan and 2 (6.7%) underwent a parathyroid CT prior to parathyroidectomy. Additionally, knowledge of the enlarged parathyroid(s) on prior imaging might have allowed a more focused approach in 3 (10.0%) and prevented 1 unnecessary thyroid lobectomy performed in search of disease. Similarly, localizable disease on old imaging might have prompted a more thorough exploration in 4 (13.3%) and possibly prevented missed disease and failure to cure in 3 (10.0%). We determined that viewing prior imaging could potentially change the preoperative evaluation in 70.0% of patients with localizable disease on old imaging and the operative course in 23.3%. When considering the entire cohort with relevant old contrast-enhanced imaging available, conservative estimates indicate reviewing these scans might alter the preoperative work-up in 52.5% of patients presenting with PHPT and the operative course in 17.5%.
Conclusions:The identification of enlarged parathyroid glands on imaging that predates a diagnosis of PHPT has the potential to impact the preoperative evaluation and intraoperative course of patients undergoing parathyroidectomy. When available, prior contrast-enhanced CT imaging should be reviewed prior to obtaining additional imaging or planning the operative approach.
Source of mentor’s funding or other support that funded this research: None
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy