 CLOSE SIDEBAR
CLOSE SIDEBAR
Outcomes of Patients with Oral Cavity Malignancies Invading the Skin
Sharon Thomson
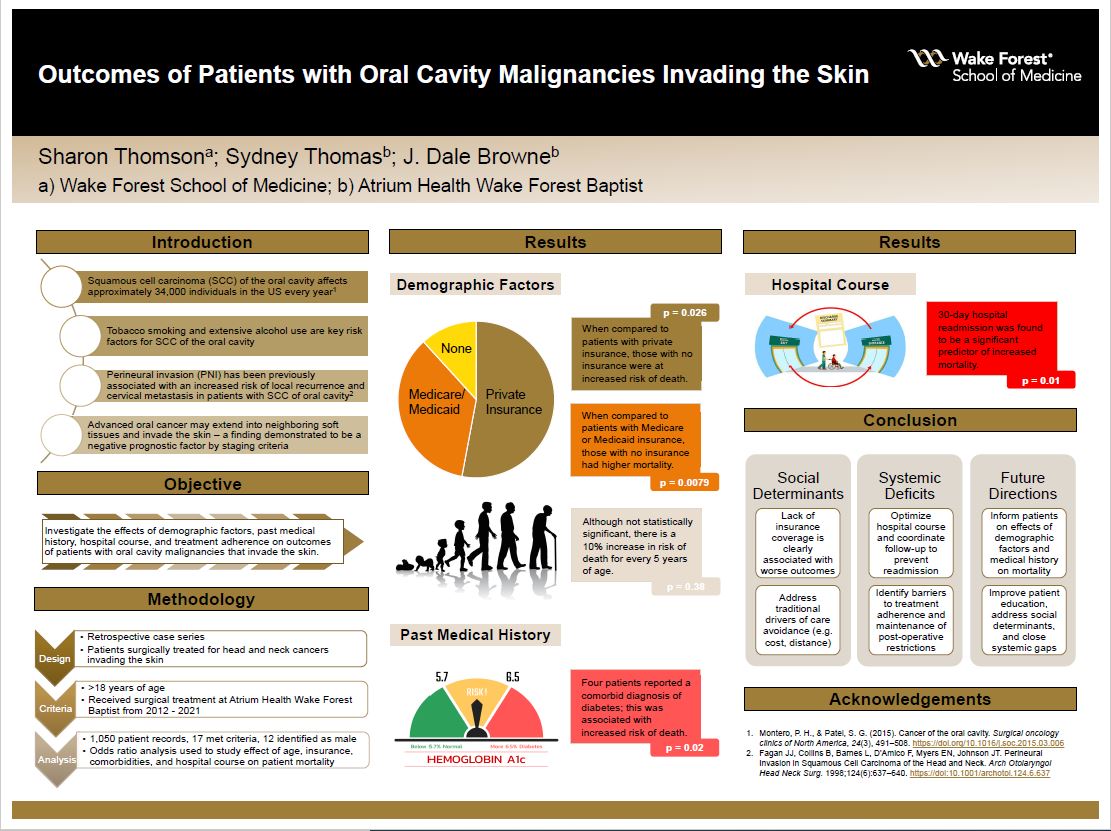
Background: Squamous cell carcinoma (SCC) of the oral cavity affects approximately 34,000 individuals, usually age > 50, in the United States every year.1 Tobacco smoking and alcohol use are key risk factors. Previous studies have established that perineural invasion (PNI) of small nerves is associated with an increased risk of local recurrence and cervical metastasis in patients with SCC of the oral cavity, oropharynx and hypopharynx, or larynx.2 Less commonly, advanced oral cancer can extend into neighboring soft tissues and invade the overlying skin; this finding has demonstrated to be a negative prognostic factor by staging criteria. Few studies have investigated the effects of age, insurance coverage, presence of comorbidities, lymphovascular invasion (LVI), 30-day hospital readmission, and completion of prescribed therapy, on outcomes of those patients with advanced oral cavity malignancies that invade the skin.
Hypothesis: We hypothesize that demographic factors such as advanced age and lack of insurance coverage would contribute to an increase in patient mortality in this subset of patients with skin invasion. We predict that clinical features such as tobacco use, alcohol use, presence of medical comorbidities, length of hospital stay, 30-day readmission, and incomplete adjuvant therapy would contribute to worse outcomes. Finally, we speculate that pathologic features such as PNI and LVI would be indicators of poor patient prognosis.
Methods: A retrospective case series of patients surgically treated for head and neck cancers invading the skin was conducted. Inclusion criteria of subjects was as follows: 1) > 18 years of age and 2) received surgical treatment for oral cavity cancer invading the skin at Atrium Health Wake Forest Baptist from 2012 – 2021. Upon review of 1,050 patient records, 17 patients met the inclusion criteria. Odds ratio analysis was used to evaluate the effect of age, insurance coverage, tobacco use, alcohol use, comorbidities (diabetes mellitus (DM), hypertension), PNI, LVI, length of hospital stay, 30-day hospital readmission, and incomplete treatment regimen on increased risk of patient mortality.
Results: Seventeen patients met inclusion criteria for this study. The median age of patients was 61 and 12 (70.5%) patients identified as male. In this sample, 9 patients reported using private insurance, 6 patients had Medicare/Medicaid coverage, and 2 patients had no insurance coverage. When compared to patients with private insurance, those without insurance were at increased risk of death (p=0.026). Similarly, when compared to patients covered with Medicare or Medicaid, those with no insurance were at higher risk of death (p=0.0079). Four patients reported a comorbid diagnosis with DM; this comorbidity was seen to be associated with worse outcomes (p=0.02). Furthermore, 30-day hospital readmission was found to be a significant predictor of poor prognosis (p=0.01). Although not statistically significant, it is noteworthy that there was a 10% increase in risk for every 5 years of age (p=0.38) and LVI (p=0.099) was also associated with increased risk of death.
Conclusions: These study findings, specifically the lack of insurance coverage, presence of DM, and 30-day hospital readmission, were found to have a significant effect on patient mortality. While the present study was limited by sample size, these findings suggest the importance of accounting for social determinants of health such as lack of insurance coverage and systemic factors such as prevention of hospital readmission in promotion of patient health and disease-free periods.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy