 CLOSE SIDEBAR
CLOSE SIDEBAR
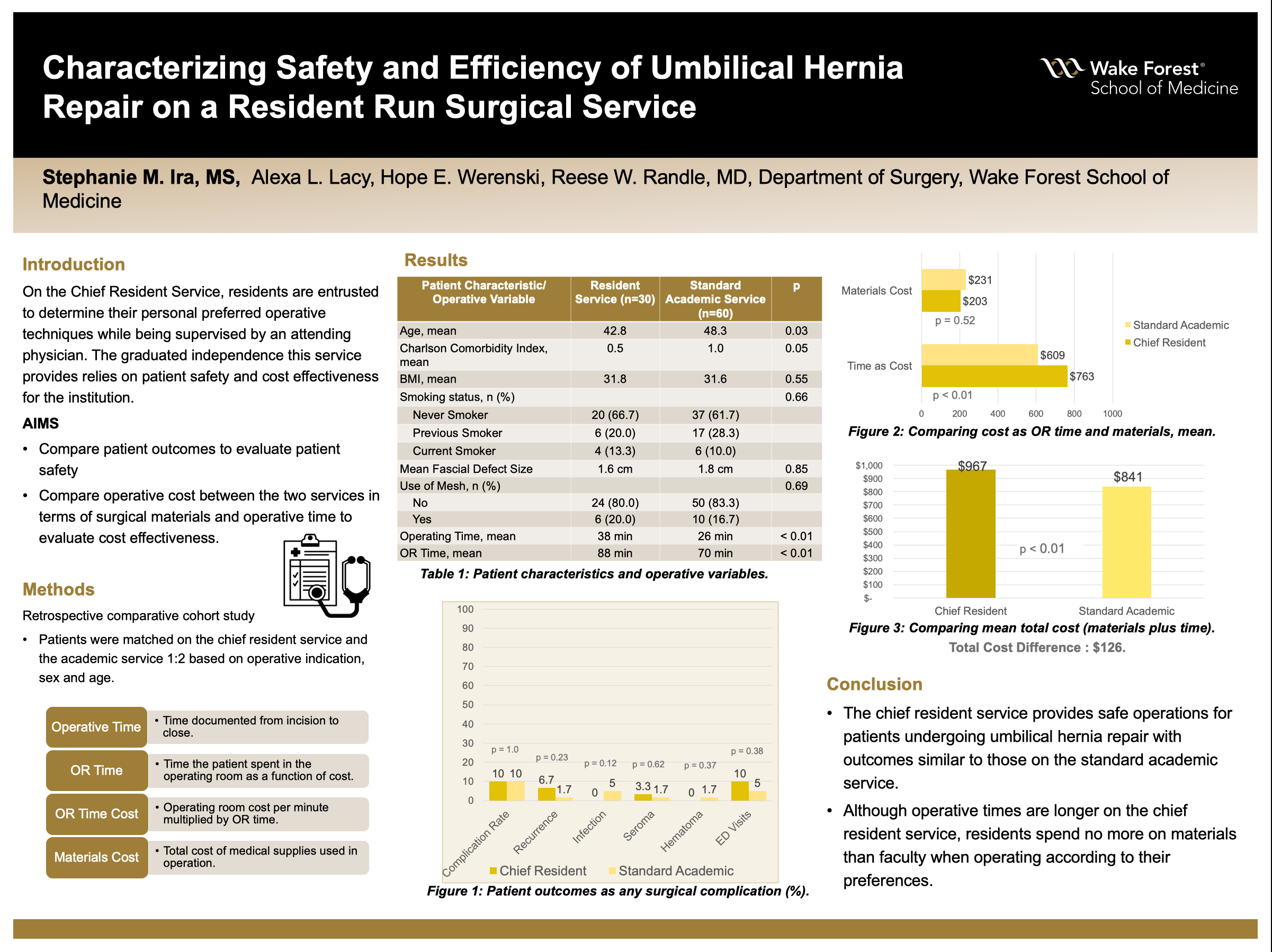
Characterizing Safety and Efficiency of Umbilical Hernia Repair on a Resident Run Surgical Service
Stephanie Ira
Background: The chief resident service provides final-year surgical trainees with a supervised experience in independence, responsibility and decision-making like they will face after graduation. Residents are entrusted to determine their personal preferred operative techniques while being supervised by an attending physician. The graduated independence this service provides is reliant on if it is safe for patients and cost effective for the institution.
Hypothesis: We hypothesized outcomes and operative cost of umbilical hernia repairs to be equivalent between the chief resident service and the standard academic service.
Methods: We matched each adult undergoing umbilical hernia repair from 07/2016-06/2019 on the chief resident service to two standard academic service patients based on operative indication, sex, and age. We compared demographics, surgical complications, operative time, 30-d complications and operative costs.
Results: This study included 90 patients undergoing open umbilical hernia repair (30 chief service patients and 60 standard academic service patients). Chief service patients had less comorbidities on average (Charlson Comorbidity Index 0.5 vs 1, P = 0.05), but mean body mass index (31.8 vs 31.6, P = .55) and fascial defect size (1.6cm vs 1.8cm, P = 0.85) were similar between the chief resident and standard academic services, respectively.
The overall complication rate was similar (10.0% chief resident, 10.0% standard, P= 1.0) Additionally, there were no significant differences in recurrence (6.7% chief resident and 1.7% standard, P = 0.23) infection (0.0% chief resident versus 5.0% standard, P= 0.12), seroma (3.3% chief resident versus 1.7% standard, P= 0.62) or hematoma (0.0% chief resident, 1.7% standard, P= 0.37) between services. Procedure-related ED visits were similar (10.0% chief resident versus 5.0% standard, P= 0.38) and no patients on either service required readmission or reoperation within 30 days.
The chief resident service averaged longer operating times (38±22 vs 26±16 min, P < 0.01) as well as more time spent in the operating room (88±34 vs 70±21 min, P <0.01) versus the standard academic service, respectively. More time in the operating room translated into higher time-based cost for chief resident’s service ($763vs $609, P < 0.01), but mean cost for materials was similar ($203vs $231, P= 0.52) between the chief resident and standard service, respectively.
Conclusions: The chief resident service provides safe operations for patients undergoing umbilical hernia repair with outcomes similar to those on the standard academic service. Although operative times are longer on the chief resident service, residents spend no more on materials than faculty when operating according to their preferences.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy