 CLOSE SIDEBAR
CLOSE SIDEBAR
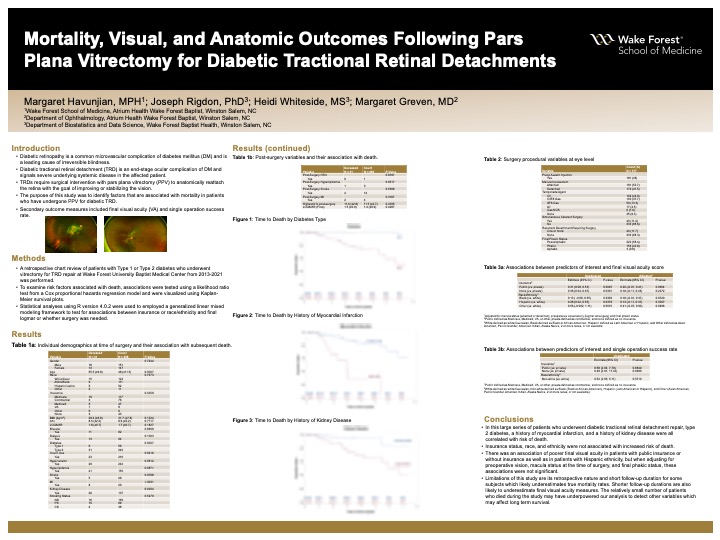
Mortality, Visual, and Anatomic Outcomes Following Pars Plana Vitrectomy for Diabetic Tractional Retinal Detachments
Margaret Havunjian
Background: By 2020, an estimated 33% of Americans will have diabetes mellitus, making it one of the largest public health challenges we face today. Diabetic retinopathy is a common microvascular complication of DM and has emerged as the leading cause of irreversible blindness in the working-age population.Vision loss due to diabetic retinopathy occurs through two main mechanisms: increased vascular permeability resulting in accumulation of intraretinal fluid and lipid (diabetic macular edema), and microvascular damage resulting in neovascularization, vitreous hemorrhage or end-stage disease, tractional retinal detachment (TRD). Patients with progressive or macula-involving diabetic TRD require surgical intervention with pars plana vitrectomy to anatomically reattach the retina with the goal of improving or stabilizing the vision.The severe microvascular disease in these patients is not limited to the eye, as significant systemic comorbidities are often present, and reduced survival has been observed in these patients compared with age-matched controls. The purpose of this study was to identify factors that are associated with mortality in patients who have undergone PPV for diabetic TRD.
Hypothesis: We hypothesize that demographic factors, medical comorbidities, visual acuity (VA) outcomes, and single operation success rates are associated with mortality rates in patients who have undergone vitrectomy to repair diabetic TRD.
Methods:A retrospective chart review of patients with type 1 or type 2 diabetes who underwent vitrectomy for TRD repair at Wake Forest University Baptist Medical Center from 2013-2021 was performed. Patient demographics, baseline data, surgical data, and post-operative data were extracted for analysis.
Results: A total of 298 patients and 378 eyes were included. Preliminary data show that age (p=.0007), type 2 diabetes (p=.0007), history of myocardial infarction (p<.0001), and history of renal disease (p=.0004) are associated with higher mortality rates in this cohort. No differences were found in race, gender, insurance status, pre-operative visual acuity, use of dialysis, insulin use, smoking status, and bilaterality of disease when comparing deceased and alive groups. Mean pre-operative VA was 1.66LogMar (Snellen) and mean post-operative VA was 1.44LogMAR (Snellen). Single operating success rate was 88.3%.
Conclusions: Age, type 2 diabetes, history of myocardial infarction, and history of renal disease are associated with mortality in patients who have undergone PPV for diabetic TRD. Further analysis of data is ongoing to determine differences in the surgical characteristics, final VA, and single operation success rate between deceased and alive patients in this cohort.
Source of mentor’s funding or other support that funded this research: The project described was supported by the National Institute of Diabetes and Digestive and Kidney Diseases, T35 Training Grant DK007400
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy