 CLOSE SIDEBAR
CLOSE SIDEBAR
The Role of Social Determinants in Post-Sepsis Readmission and Mortality: A systematic review
Ryan Hilton
ABSTRACT
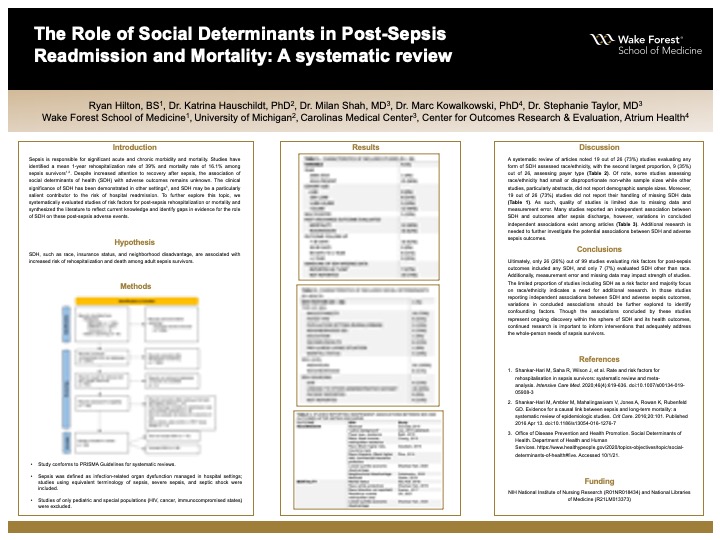
Background: Sepsis, life-threatening organ dysfunction caused by a dysregulated host response to infection, is responsible for significant acute and chronic morbidity and mortality. Sepsis survivors experience a 1-year rehospitalization rate of nearly 40% and a 1-year post-discharge mortality rate of more than 15%. Despite recent increased attention to recovery after sepsis, an important topic that remains unknown is the association of social determinants of health (SDH) with adverse outcomes. The clinical importance of SDH has been demonstrated in numerous other settings, and SDH may be a particularly salient contributor to the risk of hospital readmission. We found no systematic reviews to date that explore the relationship between SDH and risk for rehospitalization or mortality after sepsis in adults. The objective of this study was to systematically evaluate studies of risk factors for post-sepsis rehospitalization or mortality and synthesize the literature to reflect current knowledge and identify gaps in evidence for the role of SDH on these post-sepsis adverse events.
Hypothesis: SDH, such as race, insurance status, and neighborhood disadvantage, are associated with increased risk of rehospitalization and death among adult sepsis survivors.
Methods: We conducted a systematic search of MEDLINE, Cochrane Library, and EMBASE. Independent double-data extraction was following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. Studies were included if 1) the primary cohort comprised patients hospitalized with sepsis, 2) the primary outcome was rehospitalization or mortality occurring after index hospitalization for sepsis, and 3) the study assessed risk factors for these outcomes. Out of eligible studies, we determined the proportion of studies that included SDH as potential risk factors for post-sepsis outcomes and evaluated the quality of measurement of SDH. We synthesized data to report which social determinants were found to be associated with post-sepsis rehospitalization or mortality.
Results: 2,073 articles were retrieved from databases. Of 99 that met screening criteria, 26 (26%) included SDH as a potential risk factor for adverse post-sepsis outcomes, whereas 73 (74%) failed to include SDH factors. Of studies that included any SDH, the most common SDH was race/ethnicity in 19 (73%) studies. 9 (35%) studies included insurance type, 6 (23%) included income or wealth, and 5 (19%) included neighborhood socioeconomic status. Most of SDH data were obtained from electronic health records or registry linkage with information about data validation and handling of missing data often not reported. Studies reported mixed findings regarding the association between various SDH and post-sepsis outcomes.
Conclusions: Despite the clinical importance of SDH in health outcomes, only 26 (26%) out of 99 studies evaluating risk factors for post-sepsis outcomes included any SDH, and only 7 (7%) evaluated SDH other than race/ethnicity. The quality of studies is limited by lack of reporting on measurement error and missing data for SDH. Improved understanding of the social determinants that impact adverse outcomes after sepsis is important to inform interventions that adequately address the whole-person needs of sepsis survivors.
Source of mentor’s funding or other support that funded this research: NIH National Institute of Nursing Research (R01NR018434) and National Libraries of Medicine (R21LM013373)
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy