 CLOSE SIDEBAR
CLOSE SIDEBAR
Prognostic Significance of Focal and Multifocal Positive Surgical Margins Following Robotic-Assisted Radical Prostatectomy among African American Men
Bridget Krol
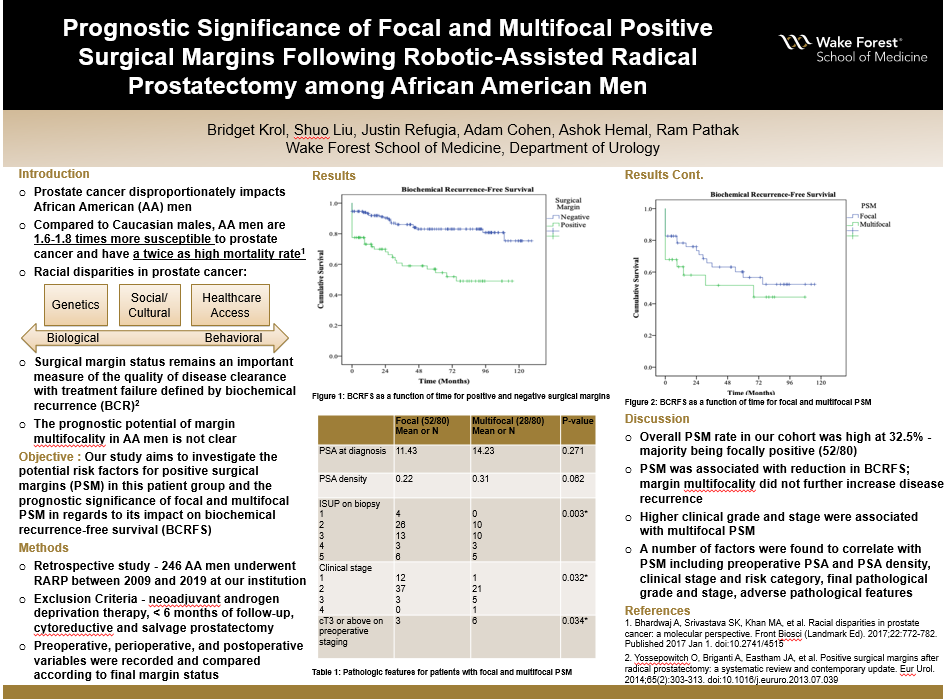
Background: Prostate cancer is the second leading cause of death in men and this disease disproportionately impacts African American (AA) males. Compared to Caucasian males, AA men are 1.6-1.8 times more susceptible to prostate cancer and have a twice as high mortality rate. The racial disparities seen in prostate cancer are likely due to cultural and socioeconomic factors, inequality in healthcare access, and differences in preventative health factors - such as awareness and motivation for prostate cancer screening. A growing body of evidence now suggests that differences at the genetic and molecular level could be more crucial than previously thought as AA men have been shown to have more aggressive tumor biology. In this era of robotic-assisted radical prostatectomy (RARP), margin status remains an important measure of the quality of disease clearance with treatment failure defined by biochemical recurrence (BCR). Unfortunately, historical series have shown that AA men tend to fare worse in this metric comparing to other ethnicities. Furthermore, the prognostic potential of margin multifocality in this population is not clear. Our study aims to investigate the potential risk factors for PSM in this patient group and the prognostic significance of focal and multifocal PSM in regards to its impact on biochemical recurrence-free survival (BCRFS).
Hypothesis: It is hypothesized that multifocal positive surgical margins will further reduce BCRFS when compared to unifocal margins in African American men.
Methods: 246 AA men underwent RARP between 2009 and 2019 at our institution. Patients who had received neoadjuvant androgen deprivation therapy, less than 6 months of postsurgical follow-up, or who underwent cytoreductive and salvage prostatectomy were excluded from the final cohort. Data were retrospectively collected from medical records and preoperative patient and disease characteristics, perioperative variables, and postoperative and pathological outcomes were recorded and compared according to final margin status. Margin focality was determined by the number of sites that cancer cells had been found at the inked margin of resection, irrespective of length.
Results: Adverse pathology (pathological stage > T3, pathological ISUP > 3, or positive nodal disease) was seen in 111 AA men (45.1%). Unifocal PSM status was observed in 52 men (21.1%) and multifocal PSM in 28 men (11.4%). PSM was associated with reduction in BCRFS (log-rank p < 0.001). Margin multifocality did not further increase disease recurrence. Patients with PSM had higher preoperative PSA (p < 0.001), higher clinical risk category (p = 0.007), higher pathological grade (p = 0.002) and incidences of perineural invasion (PNI) (p < 0.001), as well as higher percentages of clinical and pathological T3 disease. When looking specifically at pT2 disease, overall PSM rate was 22.7%. Unifocal PSM status was observed in 29 men (16.4%) and multifocal PSM in 11 men (6.25%). The multifocality of the surgical margins did not impact BCRFS in pT2 disease (p = 0.267).
Conclusions: PSM rate in AA men remained high in the era of robot-assisted surgery and significantly affected BCRFS. A number of factors have been found to correlate with PSM including, preoperative PSA and PSA density, clinical stage and risk category, and final pathological grade and stage. These patients were also more likely to have other adverse pathological features. Margin multifocality did not appear to further reduce BCRFS.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy