 CLOSE SIDEBAR
CLOSE SIDEBAR
Comparative Analysis of Costs of Caring for Inpatient COVID-19 Patients and Non-COVID-19 Patients at One Academic Center
Sam Rafla
Background: The COVID-19 pandemic created unprecedented hardship for hospital systems as hospitals had to cancel elective procedures as well as take on additional costs such as new ventilators, personal protective equipment (PPE), reduced patient to patient-to-nurse ratio, and more. To combat this, congress signed the Coronavirus Aid, Relief, and Economic Security (CARES) Act which included more than $100 billion in aid for hospital systems. The purpose of our study was to compare the daily average hospital cost of inpatient management of patients with COVID-19 infection to those without.
Hypothesis: We hypothesized that the cost of caring for a patient with COVID-19 in the inpatient setting was higher than the cost of caring for a patient with similar demographics admitted to the hospital for another diagnosis
Methods: Patients were selected from Wake Forest Baptist Hospital adult inpatients admitted to the Hospital Medicine or General Medicine service from March 2020 to February 28, 2021. After applying exclusion criteria, we randomly selected 4 non-COVID patients for each COVID patient-matched by age (≤65 and >65 years) and gender (male and female) to achieve a 1:4 case-control matched dataset. The direct cost for each hospitalization was calculated by adding ‘fixed direct cost’ and ‘variable direct cost’. An average daily cost was calculated as the ‘direct cost’ divided by the ‘total length of stay in days’. Statistical analyses were performed among COVID and non-COVID groups. Mean and standard evaluation of ‘average daily cost’ was calculated between groups and a student t-test was performed for comparison. Multivariate adjusted linear regression models were used to calculate additional ‘average daily costs’ needed for the COVID 19 patient group in comparison to the non-COVID patient group.
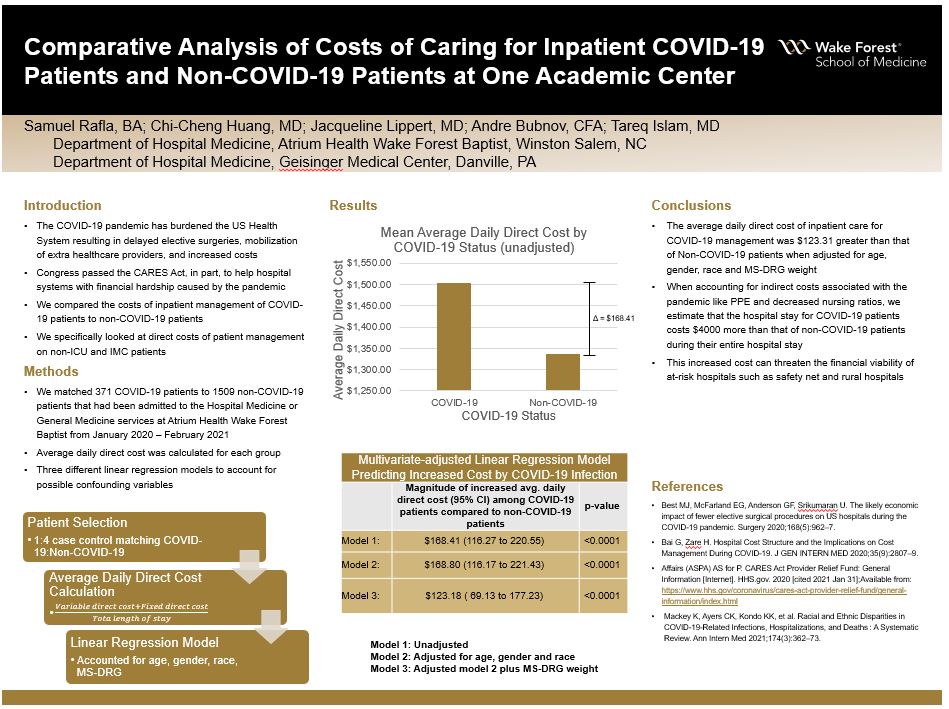
Results: After applying exclusion and inclusion criteria, the COVID-19 arm had 371 patients and the non-COVID arm had 1509 patients. The mean average daily direct cost was higher among COVID patients ($1504.4) compared to non-COVID patients ($1336.0) with statistical significance (p-value <0.001). In a multivariate-adjusted linear regression model (adjusted for age, gender, race, and MS-DRG weight), the average daily direct cost for patients with the primary diagnosis of COVID was $123.18 greater than that of non-COVID patients (p-value <0.0001).
Conclusions: Inpatient costs for COVID patients were shown to be greater than non-COVID patients. Given that we were only able to use direct costs in our model, we are likely underestimating the cost of COVID-19 patients. Examples of indirect costs that we could not include decreased nursing staff ratios, lower physician censuses, infrastructure changes (negative pressure rooms, ventilation/HVAC upgrades), and the cost of personal protective equipment (masks, gowns, gloves). These factors would likely increase the disparity in cost between the two groups. Our study’s increased costs for COVID patients highlight the financial benefit that the CARES Act provided for hospitals and healthcare systems across the country.
Source of mentor’s funding or other support that funded this research: None
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy