 CLOSE SIDEBAR
CLOSE SIDEBAR
Validation of the FUNC Score for predicting rehabilitation outcomes and eventual disposition for patients admitted with non-traumatic ICH in the inpatient rehabilitation setting
Zackary Park
Poster Title: Validation of the FUNC Score for predicting functional outcomes and eventual disposition for patients admitted with non-traumatic ICH in the inpatient rehabilitation setting
Student: Zackary Park, Class of 2024
Faculty Mentor and Department: Gregory Robbins, MD, Physical Medicine & Rehabilitation
Funding Source: none
Authors: Zackary Park, BS; Garrett Bullock, PhD, PT; Tyler Owens, DO; Gregory Robbins, MD
Funding Source: Clinical and Translational Science Institute of Wake Forest School of Medicine
ABSTRACT
Background: The Functional Outcome in Patients with Primary Intracerebral Hemorrhage (FUNC) score is a validated clinical assessment tool developed for the acute hospital setting to predict functional independence 90 days after a non-traumatic intracranial hemorrhage (ICH). Rather than predicting mortality, the FUNC score predicts functional outcome, which can be beneficial for patients, family members, and decision-makers whose primary concern is not the probability of survival, but the probability of survival with recovery of function. The FUNC score has been validated to accurately identify patients with ICH at hospital admission who are likely to achieve long-term functional independence at 90 days and those who have an ultra-low chance of functional neurological recovery at discharge. However, there is no literature that has validated the FUNC score in an inpatient rehabilitation setting. Validation of the FUNC score in an inpatient rehabilitation setting could allow medical teams to provide a more accurate prediction of functional independence and eventual disposition in patients with ICH on a much shorter time scale, which could help to guide discharge planning.
Hypothesis: We hypothesized that FUNC score should predict functional outcomes and discharge disposition for patients admitted to inpatient rehabilitation facilities after a non-traumatic intra-parenchymal hemorrhage.
Methods: We retrospectively reviewed discharges of patients with ICH from two inpatient rehabilitation centers from 2017 to 2021. FUNC score was calculated using ICH volume measured by two independent examiners, age, ICH location, Glasgow Coma Scale (GCS) score, and pre-ICH cognitive impairment. Demographic information, initial NIHSS, and comorbidities were also recorded. Logistic regressions with 95% confidence intervals and Receiver operating characteristic (AUC) curves examining the associations of combined admission AM-PAC (BM+DA) and FUNC on discharge status were performed.
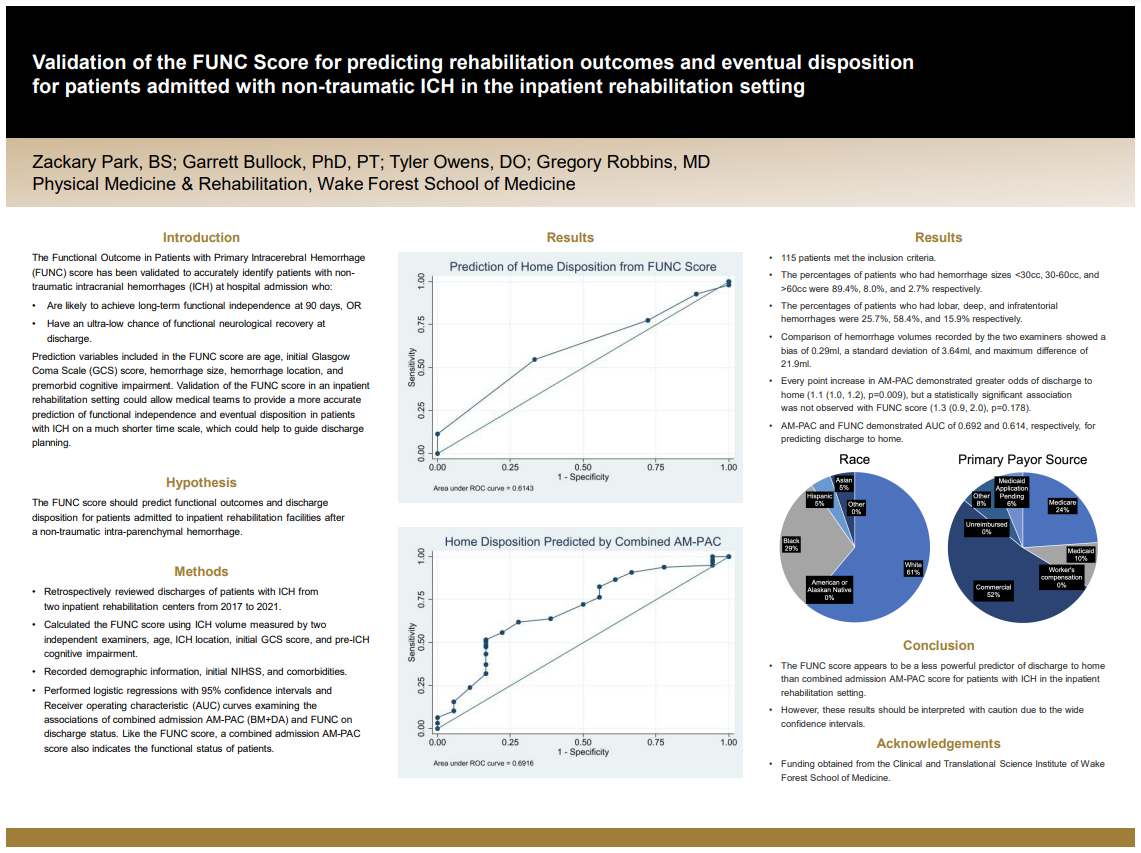
Results: 115 patients met the inclusion criteria. The percentages of patients who had hemorrhage sizes <30cc, 30-60cc, and >60cc were 89.4%, 8.0%, and 2.7% respectively. The percentages of patients who had lobar, deep, and infratentorial hemorrhages were 25.7%, 58.4%, and 15.9% respectively. Comparison of hemorrhage volumes recorded by the two examiners showed a bias of 0.29ml, a standard deviation of 3.64ml, and maximum difference of 21.9ml. Every point increase in AM-PAC demonstrated greater odds of discharge to home (1.1 (1.0, 1.2), p=0.009), but a statistically significant association was not observed with FUNC score (1.3 (0.9, 2.0), p=0.178). AM-PAC and FUNC demonstrated AUC of 0.692 and 0.614, respectively, for predicting discharge to home.
Conclusions: The FUNC score appears to be a less powerful predictor of discharge to home than combined admission AM-PAC score for patients with ICH in the inpatient rehabilitation setting. However, these results should be interpreted with caution due to the wide confidence intervals.
Source of mentor’s funding or other support that funded this research: none
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy