 CLOSE SIDEBAR
CLOSE SIDEBAR
Short- and long-term outcomes in retransplanted elderly kidney recipients
Abdu Roussi
ABSTRACT
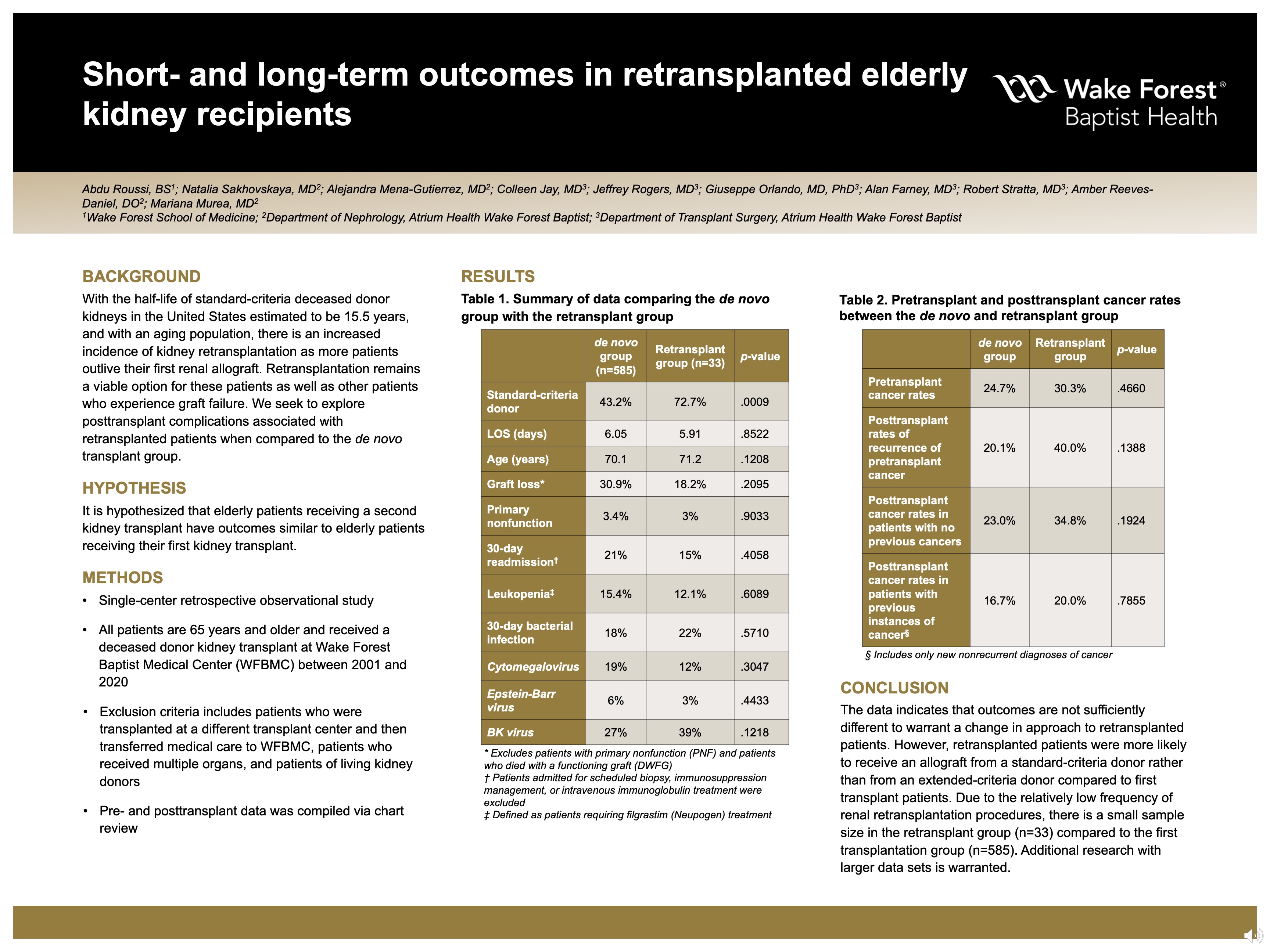
Background: With the half-life of standard-criteria deceased donor kidneys in the United States estimated to be 15.5 years, and with an aging population, there is an increased incidence of kidney retransplantation as more patients outlive their first renal allograft. Retransplantation remains a viable option for these patients as well as other patients who experience graft failure.
Hypothesis: It is hypothesized that elderly patients receiving a second kidney transplant have outcomes similar to elderly patients receiving their first kidney transplant.
Methods: This project is a single-center retrospective observational study. All patients are 65 years and older and received a deceased donor kidney transplant at Wake Forest Baptist Medical Center (WFBMC) between 2001 and 2020. Exclusion criteria includes patients who were transplanted at a different transplant center and then transferred medical care to WFBMC, patients who received multiple organs, and patients of living kidney donors. Pre- and posttransplant data was compiled via chart review.
Results: 618 patients were identified, 585 receiving their first kidney transplant and 33 retransplanted patients. Retransplanted patients were more likely to receive an allograft from a standard-criteria donor rather than an extended-criteria donor when compared to first transplant patients (72.7% vs 43.2%, p=.00089). Length of stay for first transplant and retransplanted patients was 6.05 days and 5.91 days (p=.852), respectively. Age at transplantation was 70.1 years and 71.2 years (p=.121). 30-day readmission rates were 21% and 15% (p=.406). Patients admitted for scheduled biopsy, immunosuppression management, or intravenous immunoglobulin treatment were excluded. 30-day bacterial infection rates were 18% and 22% (p=.571). Furthermore, there was also no statistically significant difference between the two groups with respect to: incidences of viremia, primary graft nonfunction, incidences of leukopenia, pretransplant and posttransplant cancer rates, and graft loss occurrence.
Conclusions: We seek to provide the perspective of a single institution with respect to outcomes of first transplant patients and retransplanted patients. The data indicates that outcomes are not different enough to warrant a change in approach to retransplanted patients. However, retransplanted patients were more likely to receive an allograft from a standard-criteria donor rather than from an extended-criteria donor compared to first transplant patients. Due to the relatively low frequency of renal retransplantation procedures, there is a small sample size in the retransplant group (n=33) compared to the first transplantation group (n=585). Additional research with larger data sets is warranted.
Source of mentor’s funding or other support that funded this research: none
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy