 CLOSE SIDEBAR
CLOSE SIDEBAR
Cost Consciousness of General Surgery Residents During Laparoscopic Cholecystectomy and Open Inguinal Hernia Repair
Alexa L. Lacy
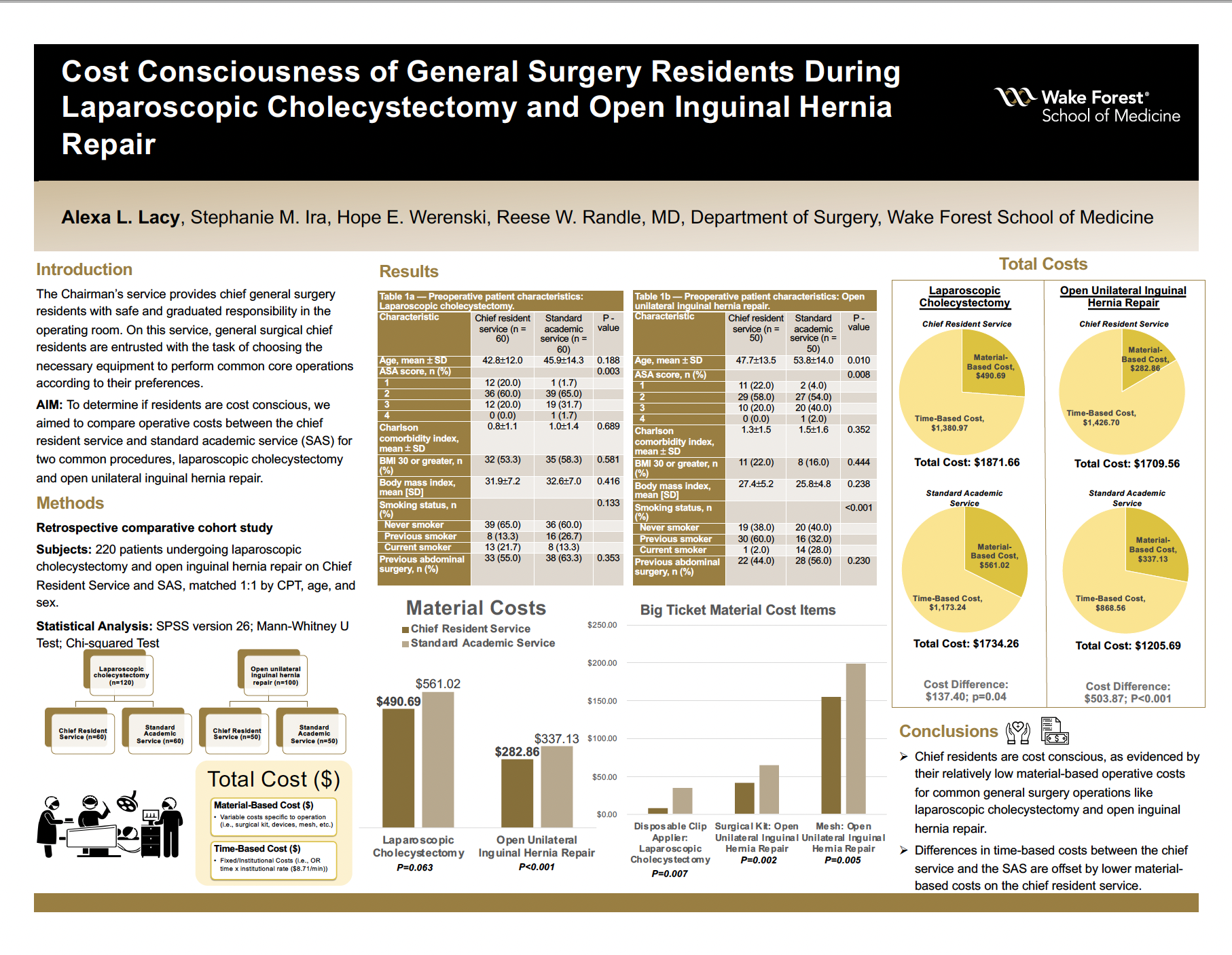
Background: General surgical chief residents are entrusted with the task of choosing the necessary equipment to perform common core operations according to their preferences on the chief resident service. To determine if residents are cost conscious when selecting the materials needed to perform these operations, we aimed to compare operative costs between the chief resident service and standard academic service (SAS) for two common procedures, laparoscopic cholecystectomy and open inguinal hernia repair.
Hypothesis: We hypothesized that chief residents will not incur higher material costs than general surgery faculty on standard academic services when they are entrusted to direct laparoscopic cholecystectomies and open inguinal hernia repairs according to their preferences.
Methods: We matched adults undergoing laparoscopic cholecystectomy and unilateral open inguinal hernia repair without additional procedures from 07/2016-06/2019 on the chief resident service to the SAS (1:1) by CPT, age, and sex. We compared material and time-based operative costs between the services.
Results: For laparoscopic cholecystectomy (n=120), body mass index (mean 31.9 versus 32.6, P=0.42), Charlson comorbidity index (mean 0.78 versus 0.98, P=0.69), and previous abdominal surgery (55% versus 63.3%, P=0.35) were similar between the chief service and SAS, respectively. Time in the operating room was greater for the chief service versus SAS (158.55 versus 134.70 minutes, P=0.001), and consequently time-based costs were greater on the chief service ($1380.97 versus $1173.24, P=0.001). However, material-based costs were lower on the chief service by an average difference of $70.33 ($490.69 versus $561.02, P=0.063). Relatedly, residents used less disposable clip appliers (3 clip appliers on the chief service versus 13 clip appliers on the SAS, P=0.006), for an average cost savings of $26.68 per case (P=0.007). The total operative cost (material and time-based costs) difference per laparoscopic cholecystectomy was only $137.40 ($1871.66 for the chief service versus $1734.26 for the SAS, P=0.04).
For open inguinal hernia repair (n=100), body mass index (mean 27.4 versus 25.8, P=0.24), Charlson comorbidity index (mean 1.3 versus 1.5, P=0.35), and previous abdominal surgery (44% versus 56%, P=0.23) were similar between the chief service and SAS, respectively. Use of mesh was almost unanimous between services (100% on chief service versus 98% on SAS, P=0.24); however, the residents used less costly mesh on average ($155.40 versus $199.30, P=0.01). The chief service had greater operating room time (163.80 versus 99.72 minutes, P=<0.001), time-based costs ($1426.7 versus $868.56, P=<0.001), and total cost ($1709.56 versus $1205.69, P=<0.001), respectively. However, chief residents spent significantly less ($282.86 versus $337.13, P=<0.001) on materials.
Conclusions: Chief residents are seemingly cost conscious as evidenced by their relatively low material-based operative costs for common general surgery operations like laparoscopic cholecystectomy and open inguinal hernia repair. Differences in time-based costs between the chief service and the SAS are offset by lower material-based costs on the chief resident service.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy