 CLOSE SIDEBAR
CLOSE SIDEBAR
COVID-19 in Older Adults With and Without Pre-Infection Neurocognitive Impairment
Bryce Polascik
Poster Title: COVID-19 in older adults with and without pre-infection neurocognitive impairment
Student: Bryce Polascik, Class of 2025
Faculty Mentor and Department: Andrew J. Liu, M.D., Duke Department of Neurology
Funding Source: None.
ABSTRACT
Background: Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) infection has been associated with significant morbidity and mortality, including central nervous system (CNS) involvement that ranges from acute delirium to meningoencephalitis during acute infection. While acute neurological manifestations have been well-described, long-term cognitive and neurobehavioral outcomes remain poorly characterized in convalescent COVID-19 patients, particularly in older adult patients with pre-existing cognitive impairment. Characterizing any neurologic, neurobehavioral, and cognitive phenotypes of COVID-19 during their convalescence is important since 80% recover, yet the relationship between exacerbated cognitive and neurobehavioral dysfunction and SARS-CoV-2 infection remains unclear. We describe shared and differing clinical characteristics of 3 older adults (aged > 65 years) who reported worsening of cognitive and neurobehavioral symptoms in the convalescent period following COVID-19.
Hypothesis: COVID-19 infection in older adults contributes to worsening of pre-existing neurocognitive impairment.
Methods: Three adults aged > 65 evaluated in the Memory Clinic of the Duke Neurological Disorders Clinic noted worsening neurocognitive difficulties after COVID-19. Electronic medical records were retrospectively reviewed. Exam included a comprehensive neurological evaluation and neuroimaging. Prior history was collected for comparison.
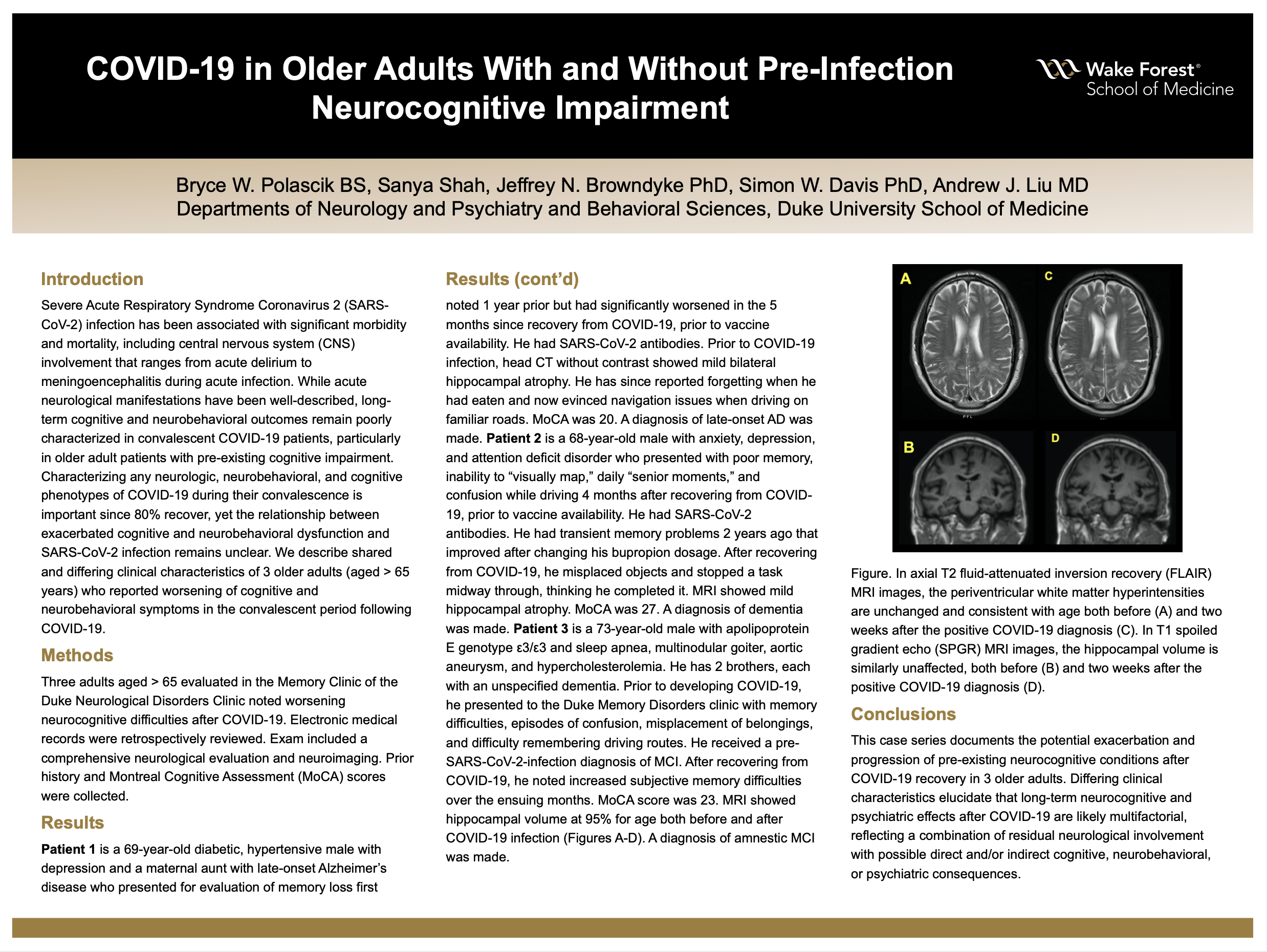
Results: Patient 1 is a 69-year-old diabetic, hypertensive male with depression and a maternal aunt with late-onset Alzheimer’s disease who presented for evaluation of memory loss first noted 1 year prior but had significantly worsened in the 5 months since recovery from COVID-19, prior to vaccine availability. He had SARS-CoV-2 antibodies. Prior to COVID-19 infection, head CT without contrast showed mild bilateral hippocampal atrophy. He has since reported forgetting when he had eaten and now evinced navigation issues when driving on familiar roads. MoCA was 20. A diagnosis of late-onset AD was made. Patient 2 is a 68-year-old male with anxiety, depression, and attention deficit disorder who presented with poor memory, inability to “visually map,” daily “senior moments,” and confusion while driving 4 months after recovering from COVID-19, prior to vaccine availability. He had SARS-CoV-2 antibodies. He had transient memory problems 2 years ago that improved after changing his bupropion dosage. After recovering from COVID-19, he misplaced objects and stopped a task midway through, thinking he completed it. MRI showed mild hippocampal atrophy. MoCA was 27. A diagnosis of dementia was made. Patient 3 is a 73-year-old male with apolipoprotein E genotype ε3/ε3 and sleep apnea, multinodular goiter, aortic aneurysm, and hypercholesterolemia. He has 2 brothers, each with an unspecified dementia. Prior to developing COVID-19, he presented to the Duke Memory Disorders clinic with memory difficulties, episodes of confusion, misplacement of belongings, and difficulty remembering driving routes. He received a pre-SARS-CoV-2-infection diagnosis of MCI. After recovering from COVID-19, he noted increased subjective memory difficulties over the ensuing months. MoCA score was 23. MRI showed hippocampal volume at 95% for age. A diagnosis of amnestic MCI was made.
Conclusions: This case series documents the potential exacerbation and progression of pre-existing neurocognitive conditions after COVID-19 recovery in 3 older adults. Differing clinical characteristics elucidate that long-term neurocognitive and psychiatric effects after COVID-19 are likely multifactorial, reflecting a combination of residual neurological involvement with possible direct and/or indirect cognitive, neurobehavioral, or psychiatric consequences.
Source of mentor’s funding or other support that funded this research: None.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy