 CLOSE SIDEBAR
CLOSE SIDEBAR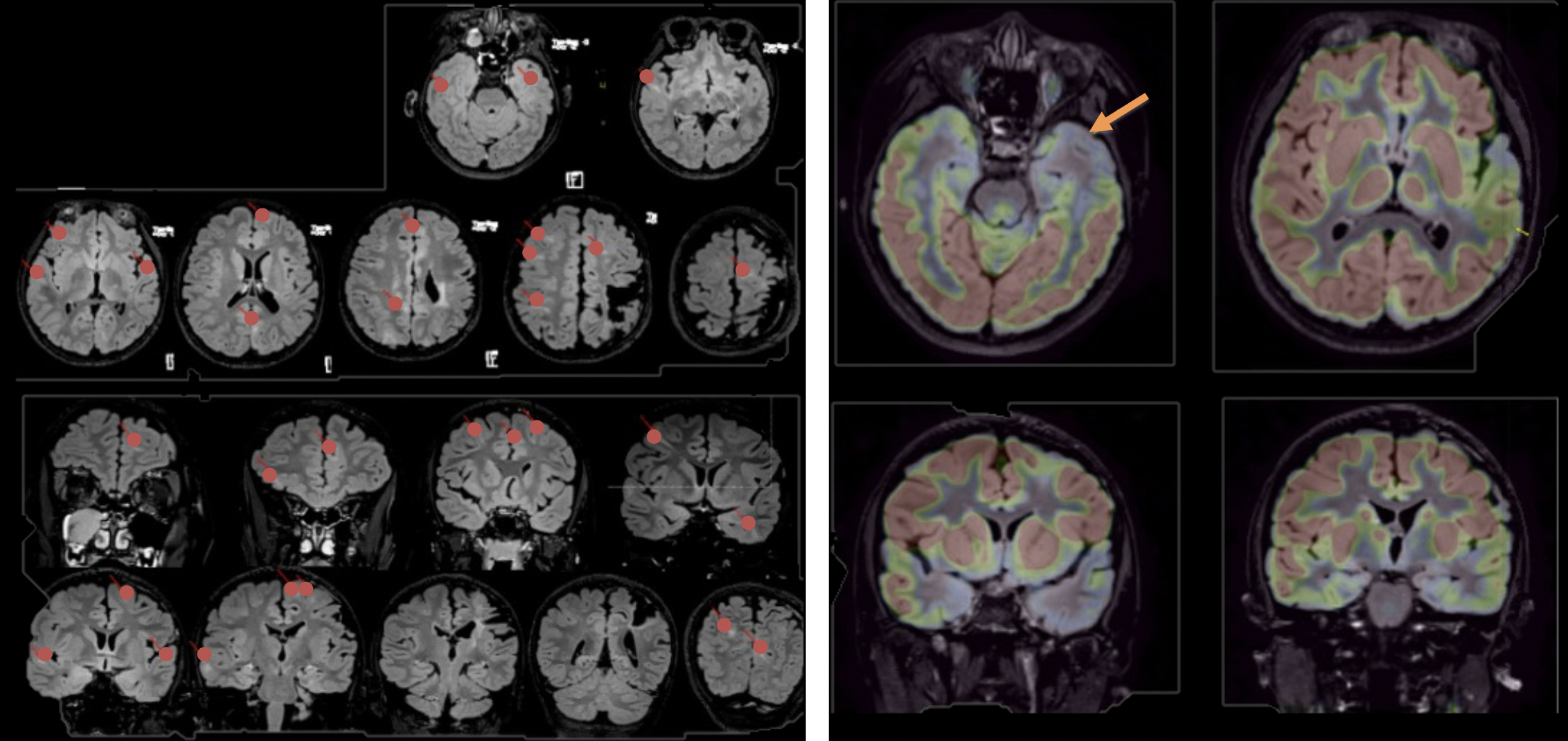
The Path to Epilepsy Surgery for a Pediatric Patient with Tuberous Sclerosis Complex and Autism Spectrum Disorder: A Case Study
Abstract:
Background: Tuberous sclerosis complex (TSC) is a rare genetic disorder that causes benign tumors (tubers) to develop in many parts of the body. Patients with TSC are at high risk for developing drug-resistant epilepsy (DRE) due to brain tubers. TSC is also associated with increased vulnerability to cognitive problems and autism spectrum disorder. For patients with DRE, epilepsy surgery may be the last hope for seizure control. The best candidates for epilepsy surgery are those with focal lesions that are consistent with seizure onset zone. Surgical candidacy is determined through a variety of procedures such as MRI, PET, long-term video EEG monitoring, neuropsychological evaluation, and stereoencephalography (SEEG).
Methods: At time of presentation to our epilepsy center, the patient was an 11-year-old, left-handed male with a history of TSC, Autism Spectrum Disorder, and drug-resistant complex partial epilepsy. He underwent previous epilepsy surgery during his first year of life after which seizures returned. He was worked up for a second epilepsy surgery, which included MRI, long-term video EEG monitoring, and neuropsychological evaluation. He also underwent SEEG to monitor habitual seizures and to cortically map cognitive function.
Results: MRI findings showed cortical and subcortical tubers and were consistent with his history of partial left frontal-parietal resection during infancy. PET showed the largest area of hypometabolism in the left anterior temporal pole and temporal cortex. EEG was abnormal due to generalized background slowing and focal epileptiform discharges in left mid-temporal and right fronto-temporal regions. Neuropsychological findings showed deficits in language and right-sided motor skill and relative strengths in nonverbal and visual-spatial skills. SEEG showed typical seizures arising from the left anterior insula and frontal operculum with rapid spread to orbital frontal and temporal pole regions. No speech/language interruptions occurred during SEEG mapping of epileptogenic zone.
Conclusion: Taken together, findings from epilepsy surgery workup identified seizure onset zone in the left anterior insula and frontal operculum and that this brain region could be resected with likely little effect on speech/language function.