 CLOSE SIDEBAR
CLOSE SIDEBAR
Comparison of Different Methodologies for Sutureless Sclerotomy Wound Closure In a Porcine Animal Model
Mallory Suarez
Background:Pars plana vitrectomies are performed using 20-, 23-, 25-, or 27-gauge instruments. Although the incisions made in pars plana vitrectomies can be constructed to be self-sealing, current methods of wound closure, including using sutures and ocular adhesives, introduce the potential for complications including incomplete sclerectomy closure, hypotony, wound leakage, endophthalmitis, ocular irritation, and granulomatous inflammation, any of which could contribute to adverse post-operative outcomes.
Hypothesis:Platelet rich plasma, whole blood, and polymerized ReSure Sealant could be utilized for clot preparation and delivery into sclerotomy incisions for sclerotomy wound closure in 23-gauge pars plana vitrectomy.
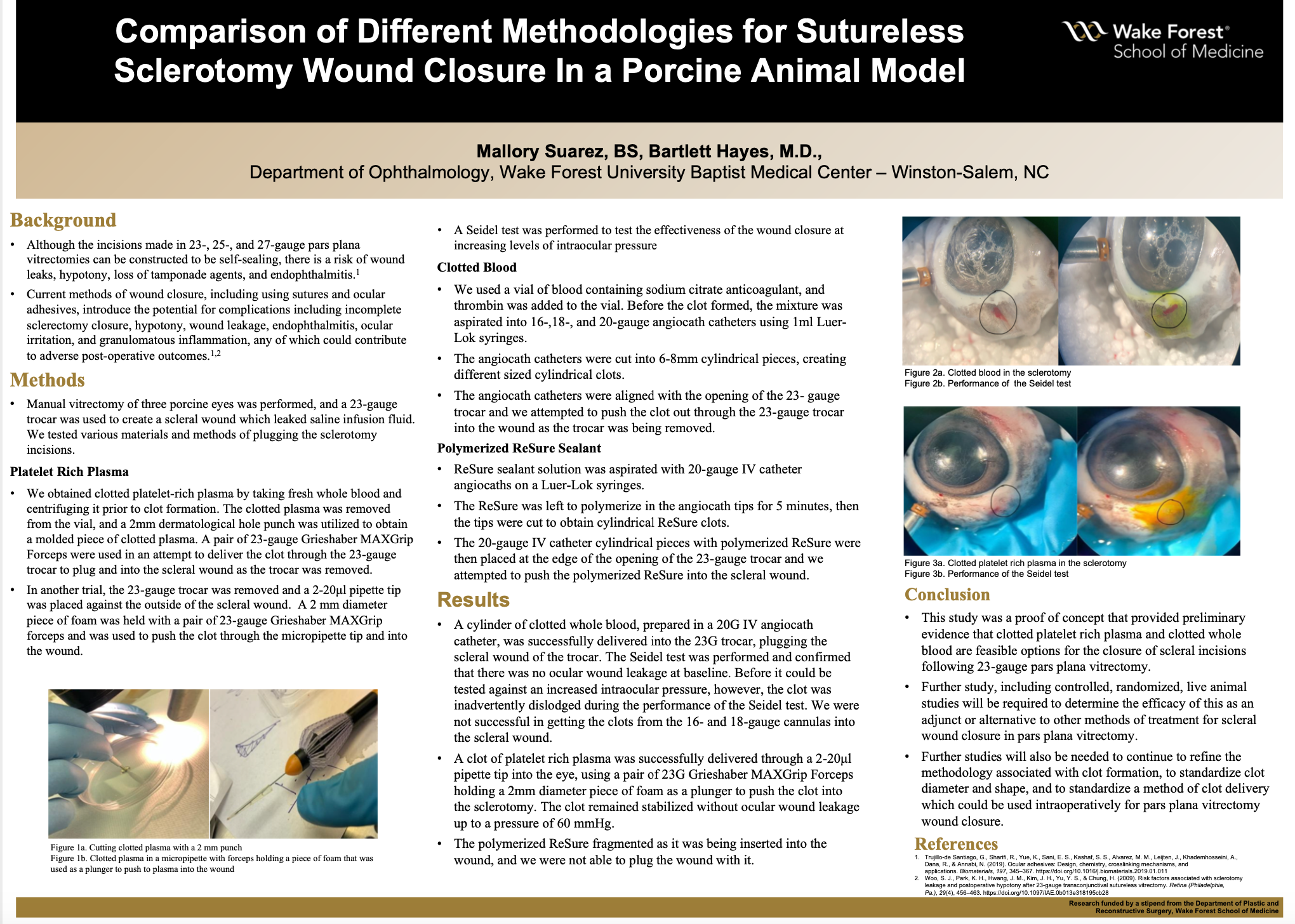
Methods:Three enucleated cadaveric porcine eyes were utilized to examine the use of different materials for sclerotomy closure. Manual vitrectomy of the porcine eye was performed, and a 23-gauge trocar was used to create a scleral wound which leaked saline infusion fluid. For PRP clot formation, 200μL of platelet rich plasma was mixed with 100μl of thrombin. In one trial, A 2mm dermatological hole punch was utilized to obtain a molded piece of clotted plasma. A pair of 23-gauge Grieshaber MAXGrip Forceps were used to deliver the clot through the 23-gauge trocar to plug the scleral wound as the trocar was removed. In another trial, we removed the 23-gauge trocar and placed a 2-20μl pipette tip up against the scleral wound to deliver the clotted plasma into the wound. We created a plunger to push the clot through the micropipette tip and into the wound by using a 2 mm diameter piece of foam held with a pair of 23-gauge Grieshaber MAXGrip Forceps. For clotted blood preparation, we utilized thrombin as a clot activator. As soon as thrombin was added to a vial of whole blood, the mixture was aspirated into 16-,18-, and 20-gauge angiocath tips on 1ml Luer-Lok syringes. The IV angiocath catheter tips were cut into 6-8mm cylindrical pieces, creating different sized cylindrical clots. The cylindrical piece of the 20G angiocath tip was aligned with the opening of the 23- gauge trocar and a 24-gauge IV angiocath was used to push the clot out through the 23-gauge trocar as it was being removed and into the scleral wound. We utilized this similar methodology of delivery to attempt to deliver polymerized ReSure Sealant through the 23-gauge trocar and into the scleral wound.
Results: In this study, the use of clotted platelet rich plasma was proven to be the most effective for scleral wound closure. In one trial utilizing platelet rich plasma, a clot was successfully delivered through a 2-20μl pipette tip into the eye, using a pair of 23G Grieshaber MAXGrip Forceps holding a 2mm diameter piece of foam as a plunger to push the clot into the sclerotomy. The effectiveness of the clot was measured using the Seidel Test at increasing intraocular pressure to evaluate for wound leakage. The clot remained stabilized without ocular wound leakage up to a pressure of 60 mmHg. In one trial with clotted whole blood, a clot prepared in a 20G IV angiocath tip was successfully delivered through the 23G trocar, plugging the scleral wound of the trocar. The Seidel test was performed and confirmed that there was no ocular wound leakage at baseline. Although the clot was successfully delivered, before it could be tested against an increased intraocular pressure, it was dislodged during the performance of the Seidel test.
Conclusions: This study was a proof of concept that provided preliminary evidence that clotted platelet rich plasma and clotted whole blood could be feasible options for the future of scleral wound closure. Further well controlled, randomized, and live animal studies will be required to determine the efficacy of this as an adjunct or alternative to other methods of treatment for scleral wound closure in pars plana vitrectomy.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy