 CLOSE SIDEBAR
CLOSE SIDEBAR
Role of Tumor Mutational Burden Comparative with PD-L1 in HNSCC
Elena Gavrila
Background: Immunotherapy with checkpoint inhibitors (ICI) prompted a dramatic progress in the management of head and neck squamous cell carcinoma (HNSCC), improving survival and raising hope for cure even in advanced stages. Disappointingly, the percentage of patients able to benefit from this progress remains limited to 20% or less. Development of Precision Oncology in HNSCC brings the prospect for emergency of biomarkers of response to immunotherapy that can help with the selection of the subset of patients that may benefit the most from treatment with ICI. As a result of these efforts, biomarkers such as TMB are currently under investigation in many solid tumors including HNSCC.
Methods: This is a single institution retrospective review of patients with HNSCC having tumor tissue evaluated for TMB by FoundationOne. PD-L1 expression determined using IHC 22C3 pharmDx kit and reported as TPS score (until 2018) and CPS score afterwards was collected. TMB and PD-L1 were analyzed for their individual association with demographics, risk factors, disease characteristics and survival, as well as for correlation with response to immunotherapy with ICI in a fraction of patients. Patients tested for TMB were grouped as TMB-low (1-5) and TMB-high (6+) and patients tested for PD-L1 were grouped as PD-L1 0, PD-L1 1-19 and PD-L1 20+. All patients included in this study had at least six months of follow up after the sample collection for TMB and/or PD-L1 testing.
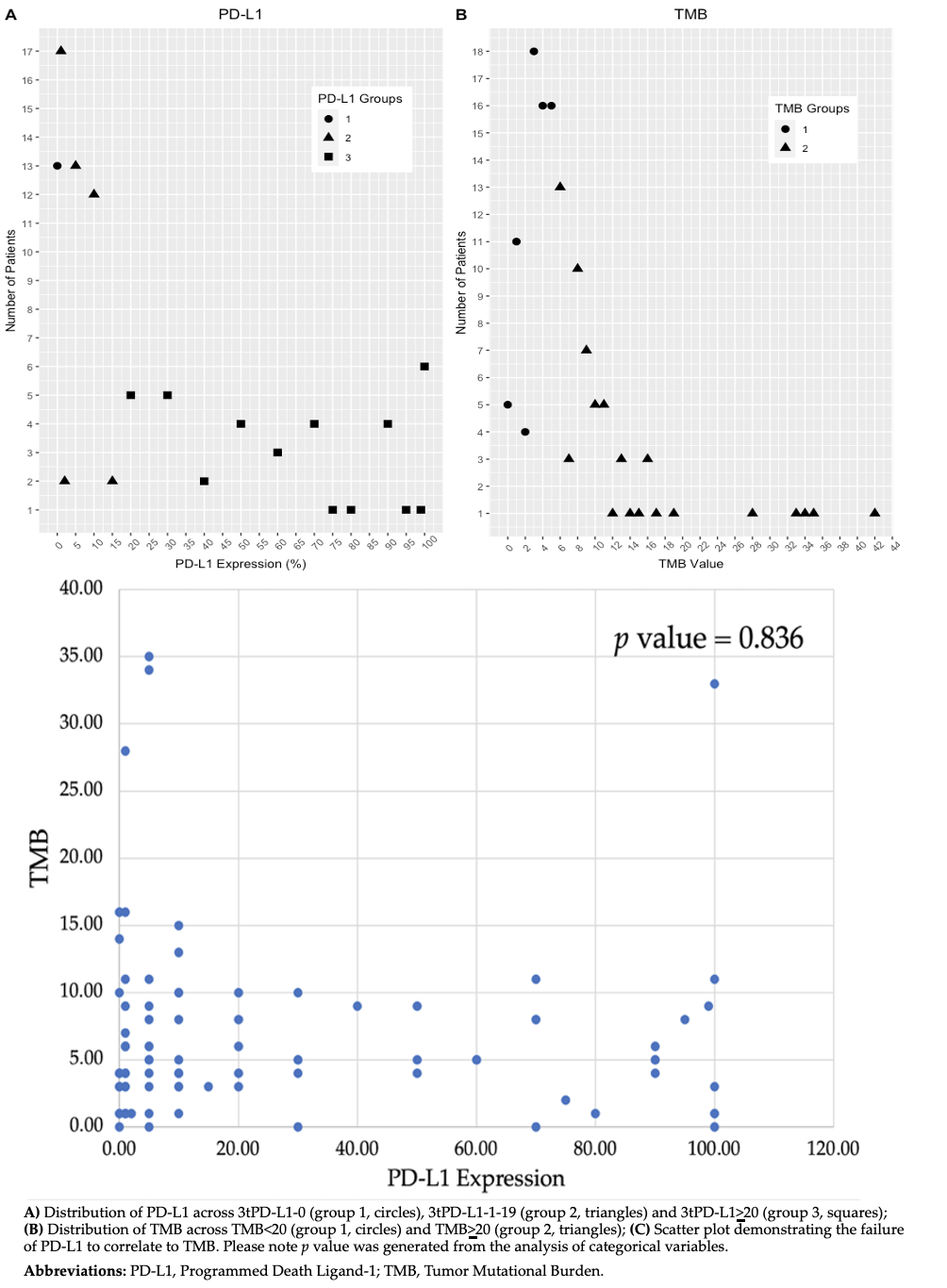
Results: Our analysis included 139 patients, of whom 128 patients had TMB, 95 patients had PD-L1 and 92 patients had both variables reported. TMB-high was found associated with smoking, (p=0.03) and tumor location (p < 0.01) with larynx patients having significantly higher TMB (p=0.006) and oropharynx patients having lower TMB (p=0.004). African Americans and patients with BMI above 30 tended to have lower TMB scores, although not reaching statistical significance (p=0.08 and p=0.07 respectively). PD-L1 was statistically significant higher in African Americans (p=0.02) and in never smokers (p=0.04) and never drinkers (p=0.01), as well as in patients with earlier cancer stage (p=0.03) and lower tumor stage (p=0.008). There was no significant correlation of TMB or PD-L1 with HPV status, however it was noted that there were no HPV-positive patients vs 18.6% of HPV negative patients with PD-L1 0.TMB was associated with survival, with patients with high TMB scores faring better in univariate analysis (p= 0.02) and in in a Cox proportional hazards regression model when adjusted for age, tobacco use, tumor site, nodal stage at diagnosis, previous treatment with chemotherapy, radiation or combined chemoradiation therapy and PD-L1 level in a multivariate analysis model (p = 0.0002). No similar correlation was found between level of PD-L1 expression and prognosis. There was no correlation found between TMB and PD-L1 level. A total of 79 patients in this study received at least one treatment with an ICI. Treatment efficacy was able to be evaluated in 51 of these patients, of whom 40 patients had TMB reported and 36 patients had PD-L1 results available. There was a statistically significant association between the response to treatment with ICI and continuous TMB score with a mean TMB of 11.2 in responders and 4.9 in tumor progressors (p=0.01). Evaluation as a categorical variable demonstrated that 66.6% of the responders and 33.3% of the progressors were within the TMB-high category (p=0.055). There was no association found between response to treatment with ICI and PD-L1 level analyzed as a categorical (p=0.89) or continues variable (mean PD-L1 was 26.4 in responders versus 26.5 in progressors; p=0.99).
Conclusions: TMB rather than PD-L1, the currently utilized marker for recommendation of treatment with ICI in HNSCC, showed significant association with survival and response to treatment with immunotherapy. Further larger studies are needed to reshape the biomarkers utilization to select patients for treatment with ICI in HNSCC. Interestingly, PD-L1 level and TMB appear to be affected oppositely by demographics (such as race) and risk factors (such as smoking) suggesting consideration for researching congregated rather than individual biomarkers in future studies.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy