 CLOSE SIDEBAR
CLOSE SIDEBAR
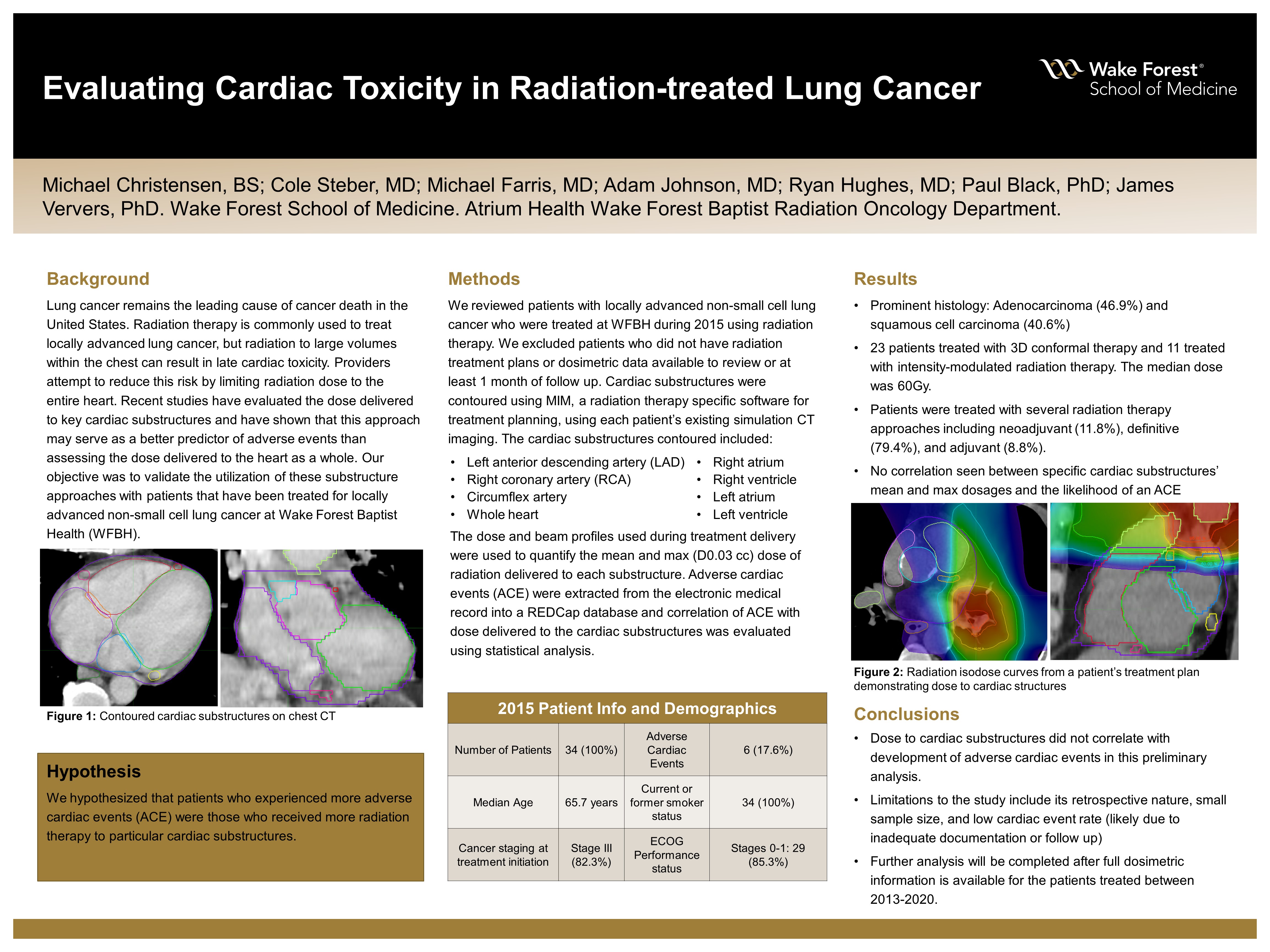
Evaluating Cardiac Toxicity in Locally Advanced Lung Cancer Treated with Chemo Radiation
Michael Christensen, BS
Poster Title: Evaluating cardiac toxicity in locally advanced lung cancer treated with chemo radiation
Student: Michael Christensen, Class of 2024
Faculty Mentor and Department: Dr. Michael Farris, Radiation Oncology
Funding Source: Kulynych Family Funds for Medical Research in Honor of Timothy C. Pennell, MD
ABSTRACT
Background: Lung cancer is the leading cause of cancer death in the United States. Radiation therapy is a modality often used in the treatment of locally advanced lung cancer, but there is extensive room for better defining the critical thresholds associated with cardiac toxicity. Recent small studies have investigated the dose delivered to key cardiac substructures and have shown that this approach may serve as a better predictor of toxicity than just assessing the dose delivered to the heart as a whole. Our objective is to validate the utilization of these substructure approaches with patients that have been treated for locally advanced non-small cell lung cancer at Wake Forest Baptist Health (WFBH).
Hypothesis: It is hypothesized that there will be more adverse cardiac events (ACE) associated with patients who received more radiation therapy to particular cardiac substructures.
Methods: We reviewed patients with locally advanced non-small cell lung cancer who were treated at WFBH during the year 2015 using radiation therapy. We excluded patients who did not have radiation treatment plans or dosimetric data available to review or at least 1 month of follow up. Cardiac substructures were contoured using MIM, a radiation therapy specific software for treatment planning, using each patient’s existing simulation CT imaging. The cardiac substructures contoured included: right atrium, right ventricle, left atrium, left ventricle, left anterior descending artery (LAD), right coronary artery (RCA), circumflex artery, and the whole heart. The actual dose and beam profiles used during treatment delivery were used to quantify the mean and max (D0.03 cc) dose of radiation delivered to each substructure. Subsequent adverse cardiac events (ACE) were extracted from an existing REDCap database and correlation of ACE with dose delivered to the cardiac substructures was evaluated using statistical analysis.
Results: Of the 34 evaluable patients with locally advanced lung cancer treated in 2015, the median age at diagnosis was 65.7 years, had ECOG 0-1 (85.2%), and all were current (35.3%) or former smokers (64.7%). All patients were staged using PET/CT, a majority were stage III (82.3%), and the predominant histology included adenocarcinoma (46.9%) or squamous cell carcinoma (40.6%). Patients were treated with several radiation therapy approaches including neoadjuvant (11.8%), definitive (79.4%), and adjuvant (8.8%). Twenty-three (67.6%) patients were treated with three-dimensional conformal therapy while 11 (32.4%) patients were treated with intensity-modulated radiation therapy, with a median dose of 60 Gy. Concurrent chemotherapy was given for 29 (85.3%) patients, induction chemotherapy for 4 (11.8%), and adjuvant chemotherapy was given for 6 (17.6%) of patients. Only four patients (11.8%) received immunotherapy. After completions of radiation therapy, 6 patients (17.6%) developed an ACE. No cardiac substructure mean or max dose was found to significantly correlate with development of ACE after radiation therapy.
Conclusions: Dose to cardiac substructures did not correlate with development of cardiac events in this preliminary analysis. This conclusion is limited due to the retrospective nature of this analysis, the small sample size included for analysis, as well as the low cardiac event rate which may be limited due to the lack of quality and reporting of such events within the electronic medical record. Further analysis will be completed after full dosimetric information is available for the patients in the time period from 2013-2020.
Source of mentor’s funding or other support that funded this research: None
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy