 CLOSE SIDEBAR
CLOSE SIDEBAR
High-Risk Breast Cancer Screening in Patients Under 40
Gregory R. Lombana
Background: Annual screening mammography is recommended to begin at age 40 for women who are at average risk of developing breast cancer. For high-risk women, earlier screening with the addition of breast MRI is preferred. Although this recommendation is well-supported, many women under the age of 40 are diagnosed with breast cancer without having undergone appropriate early screening. The actual rate of adherence to these guidelines is unclear. This study investigates our institutional utilization of appropriate screening efforts in high-risk women diagnosed with breast cancer under age 40.
Methods: A retrospective review of patients with breast cancer diagnosed before age 40 between 2013-2018 was conducted. Demographics, obstetric history, personal/family histories, biopsy/surgical details, radiologic information, and preoperative variables were collected. Patients were identified as being at increased risk of breast cancer as defined by the National Comprehensive Cancer Network (NCCN) guidelines and the Tyrer-Cuzick (TC) model (≥ 20% lifetime risk).
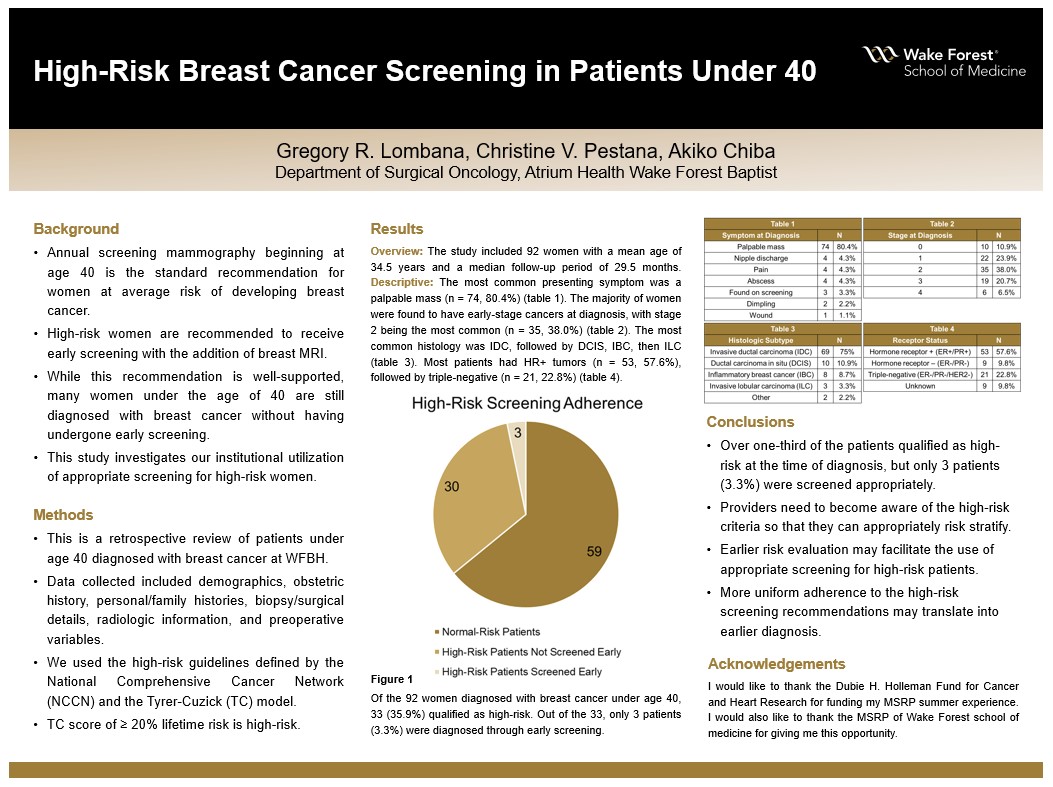
Results: The study included 92 women with a mean age of 34.5 years and a median follow-up period 29.5 months. Most subjects self-identified as non-Hispanic White women (66.3%). The most common presenting symptom was a palpable mass (n = 74, 80.4%), and the vast minority of cancers were diagnosed by screening (n = 3, 3.3%). The most common histology was invasive ductal carcinoma (IDC) (n = 69, 75%), followed by ductal carcinoma in situ (DCIS) (n = 10, 10.8%), and inflammatory breast cancer (IBC) (n = 8, 8.7%). The majority of women were found to have early-stage breast cancer, with more than 50% being diagnosed at Stage I or Stage II disease. ER/PR+ cancers (57.6%) were more common than ER/PR- cancers (37.6%), and both were more common than triple-negative breast cancer (TNBC) (22.8%). Although 35.9% of the women included met criteria for early screening per NCCN guidelines, only 3.3% (n = 3) were appropriately screened prior to their diagnosis. Almost all patients (98.9%) were offered genetic testing by their surgeon during initial consultation, and among those tested, 15.3% were found to be positive for BRCA1 or BRCA2, and 21.2% carried other pathogenic mutations.
Conclusions: Despite over one-third of this patient population qualifying as high-risk at the time of diagnosis, only 3 of them were diagnosed through implementation of high-risk screening. This discrepancy presents an opportunity to improve awareness among providers regarding how breast cancer risk is evaluated in the primary care setting. Earlier risk evaluation and identification of high-risk patients may facilitate the use of appropriate screening measures for this population, and this may translate to earlier breast cancer diagnosis.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy