 CLOSE SIDEBAR
CLOSE SIDEBAR
Response and local control in patients treated with low-dose radiotherapy for tumoral mycosis fungoides
Deborah Cull
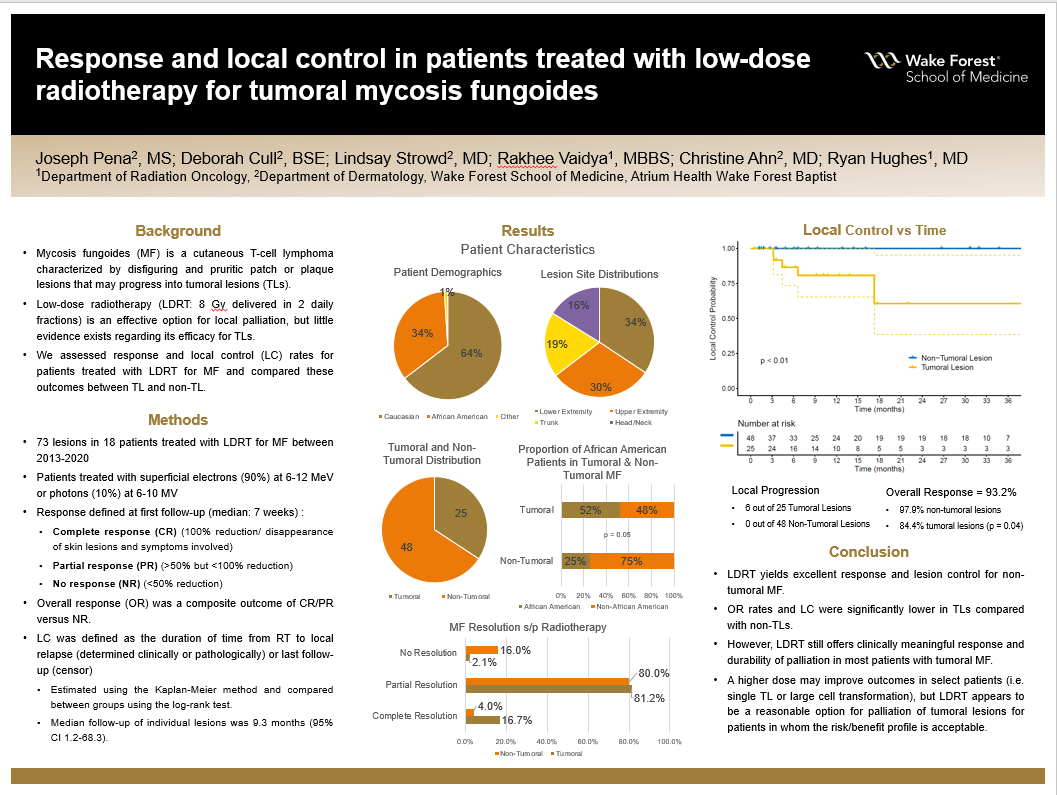
Background: Mycosis fungoides (MF) is a cutaneous T-cell lymphoma characterized by disfiguring and pruritic patch or plaque lesions that may progress into tumoral lesions (TLs). Low-dose radiotherapy (LDRT: 8 Gy delivered in 2 daily fractions) is an effective option for local palliation, but little evidence exists regarding its efficacy for TLs. We assessed response and local control (LC) rates for patients treated with LDRT for MF and compared these outcomes between TL and non-TL.
Hypothesis: It is hypothesized that low-dose radiotherapy (LDRT) is an effective option for palliation and local control in tumoral lesions (TLs).
Methods: A total of 73 lesions in 18 patients treated with LDRT for MF between 2013-2020 were analyzed. Patients were treated with superficial electrons (90%) or photons (10%) using beam energies of 6-12 MeV or 6-10 MV, respectively. Response was defined at first follow-up (median: 7 weeks) and defined as follows: complete response (CR), 100% reduction/disappearance of skin lesions and symptoms involved; partial response (PR), >50% but <100% reduction; no response (NR), <50% reduction. Overall response (OR) was a composite outcome of CR/PR versus NR. LC was defined as the duration of time from RT to local relapse (determined clinically or pathologically) or last follow-up (censor), was estimated using the Kaplan-Meier method and compared between groups using the log-rank test. Median follow-up of individual lesions was 9.3 months (95% CI 1.2-68.3).
Results: Median age was 68 years, 85% of patients were male, 64% identified as Caucasian, 34% as Black/African American (B/AA), and 1% other. Lesion site included the lower extremity (34%), upper extremity (30%), chest/abdomen/trunk (19%) and head/face/neck (16%). Of the 73 lesions, 25 were tumoral and 48 were non-tumoral. A greater proportion of B/AA race was observed in the TL group (52% TL v. 25% non-TL, p = 0.05). Five lesions had biopsy-confirmed large cell transformation, all in the TL group. OR was 93.2% overall (97.9% non-TL v. 84% TL, p = 0.04). In the non-TL versus TL groups, CR was observed in 16.7% v. 4.0%, PR in 81.2% v. 80.0%, NR in 2.1% v. 16.0%, respectively. Local progression was noted in 6/25 TL and 0/48 non-TL. LC at 6, 12, and 24 months was 100% for non-TLs compared with 86.6% (95% CI 73.4-100), 80.8% (65.3-100), and 60.6% (38.5-95.4) for TLs (p < 0.01). Median time-to-progression in the 6 TL that failed was 5.5 months (95% CI 3.2-17.3).
Conclusions: LDRT yields excellent response and lesion control for non-tumoral MF. OR rates and LC were significantly lower in TLs compared with non-TLs. However, LDRT still offers clinically meaningful response and durability of palliation in most patients with tumoral MF. A higher dose may improve outcomes in select patients (i.e. single TL or large cell transformation), but LDRT appears to be a reasonable option for palliation of tumoral lesions for patients in whom the risk/benefit profile is acceptable.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy