 CLOSE SIDEBAR
CLOSE SIDEBAR
Ethnic and Racial Breakdown of Patients with Staphylococcal Scalded Skin Syndrome
Stephanie Snyder
Background: Staphylococcal scalded skin syndrome (SSSS), also known as Ritter’s Disease, is a common dermatological condition in pediatric populations. It is caused by exfoliative toxins A and B released by the bacteria Staphylococus aureus. Following a recent infection such as otitis media, upper respiratory infection or infection of the umbilical stump, patients present appearing generally ill. A tender rash develops over the next 1-2 days, followed by blister formation. Fragile bullae form initially on the central face, neck, axillae and groin, with epidermal detachment. The toxins produced by S. aureus breakdown desmosomes in the epidermis, leading to blisters. Pediatric patients with SSSS are at risk for secondary infections, but typically progress well with supportive care and the risk of mortality is low.
Hypothesis: Limited information is available regarding the specific racial breakdown of patients with SSSS. One study focused on the epidemiology of SSSS in children and showed an inverse relationship between risk of SSSS and black race. Another study, focusing on the epidemiology of SSSS in adults, showed different results that suggested an increased risk of SSSS with black race. These studies relied on ICD 9 diagnosis codes, indicating the diagnosis was not confirmed by dermatology. More information is needed regarding the prevalence of SSSS in skin of color. Furthermore, the use of ICD- 10 codes will provide more accurate data regarding the prevalence of SSSS.
Methods: A retrospective chart review was performed using the electronic medical record. Any patient regardless of sex, age, ethnicity diagnosed with SSSS between 10/1/2010 and 5/1/2021 at select academic medical centers, who also had a formal inpatient dermatology consultation or virtual consultation with clinical images, was considered eligible for the study. The electronic medical records were evaluated for age at admission, sex, race, ethnicity, need for inpatient hospitalization, length of hospital stay, culture data, choice of initial antibiotic, choice of final antibiotic, length of antibiotic use, wound care, and post-disease sequelae.
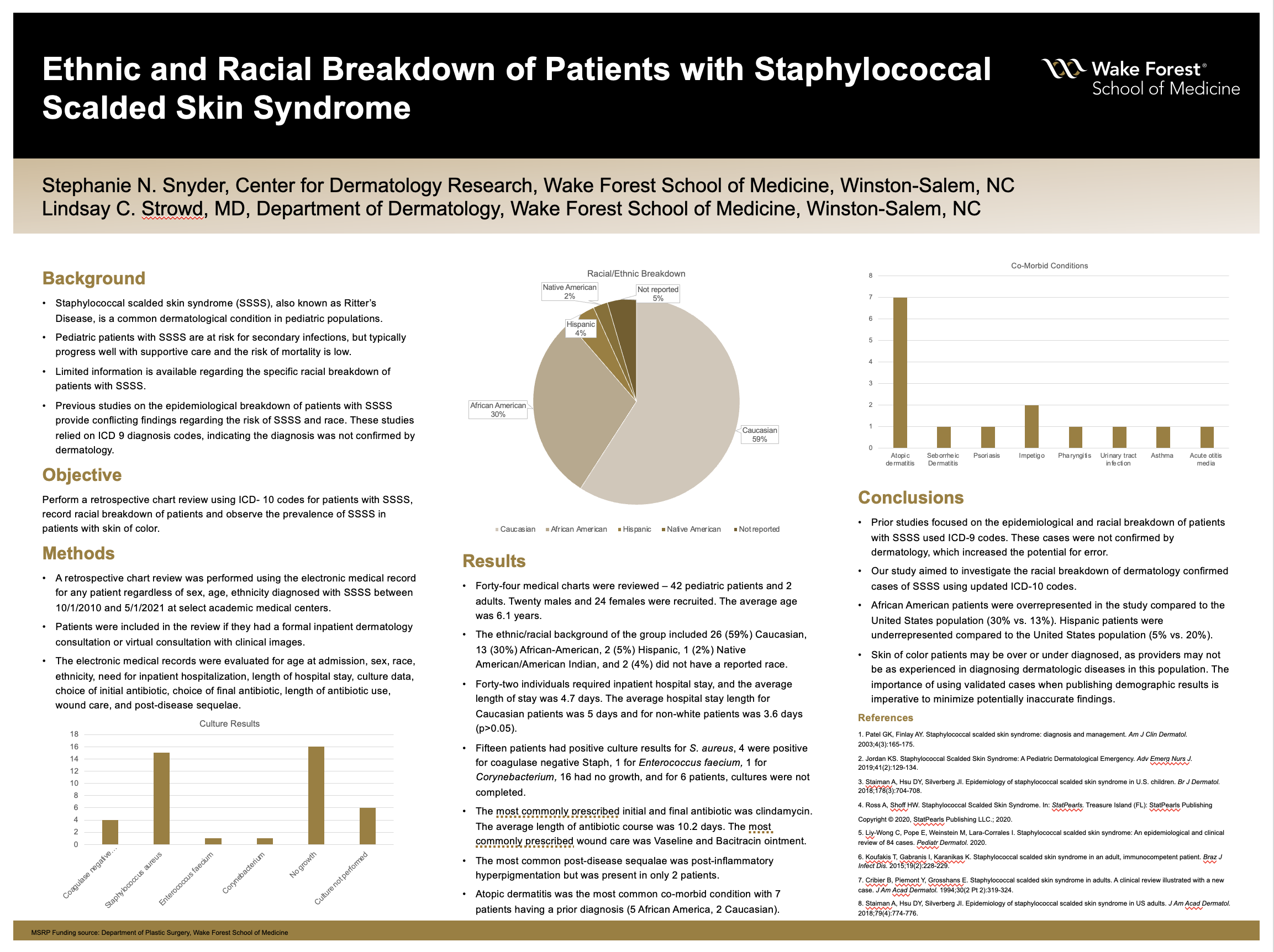
Results: Forty-four medical charts were reviewed. Twenty males and 24 females were recruited. The average age was 6.1 years. The ethnic/racial background of the group included 26 (59%) Caucasian, 13 (30%) African-American, 2 (5%) Hispanic, 1 (2%) Native American/American Indian, and 2 (4%) did not have a reported race. Forty-two individuals required inpatient hospital stay, and the average length of stay was 4.7 days. The average hospital stay length for Caucasian patients was 5 days and for non-white patients was 3.6 days (p>0.05). Fifteen patients had positive culture results for S. aureus, 4 were positive for coagulase negative Staph, 1 for Enterococcus faecium, 1 for Corynebacterium, 16 had no growth, and for 6 patients, cultures were not completed. The most commonly prescribed initial and final antibiotic was clindamycin. The average length of antibiotic course was 10.2 days. The most commonly prescribed wound care was Vaseline and Bacitracin ointment. The most common post-disease sequalae was post-inflammatory hyperpigmentation but was present in only 2 patients. Atopic dermatitis was the most common co-morbid condition with 7 patients having a prior diagnosis (5 African America, 2 Caucasian).
Conclusions: Prior studies focused on the epidemiological and racial breakdown of patients with SSSS used ICD-9 codes and national databases to observe the differences between cases of SSSS. These cases were not confirmed by dermatology, which increased the potential for error. Our study aimed to investigate the racial breakdown of dermatology confirmed cases of SSSS using updated ICD-10 codes. The majority of patients seen for SSSS in the inpatient setting were Caucasian, but African American patients were overrepresented in the study compared to the United States population (30% vs. 13%). Hispanic patients were underrepresented compared to the United States population (5% vs. 20%). The importance of using validated cases when publishing demographic results is imperative to minimize potentially inaccurate findings.
Source of mentor’s funding or other support that funded this research: None
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy