 CLOSE SIDEBAR
CLOSE SIDEBAR
HSV Central Nervous System Infections and Immune Compromise
Chiagoziem Ogbonna
ABSTRACT
Background: HSV-1 is the primary causal agent of fatal encephalitis in the United States. HSV-2 encephalitis is much less common and is typically associated with some form of immune compromise. Data on risk factors for HSV encephalitis and other CNS infections remains limited for a wide range of immunologic conditions. The aim of this study was to evaluate the epidemiology of HSV CNS infections at our hospital and to identify novel associations within specific groups of immunocompromised hosts.
Hypothesis: We hypothesized that the expanding use of immunosuppressive medications for a variety of disease processes is changing the spectrum of underlying conditions associated with HSV-1 and -2 encephalitis and other CNS infections.
Methods: From the Microbiology laboratory information system (Beaker®) we identified all positive CSF PCR tests obtained at WFBH-WS from 1/1/2015 to 12/31/2021. PCR results had been obtained using the BioFire® FilmArray® meningitis/encephalitis panel and the HSV PCR developed at the institutional laboratory. We then reviewed case data from Epic® electronic health records (EHR). A positive CSF PCR, being ≥18 y-old and sufficient information in the EHR to confirm a diagnosis of encephalitis were all required for inclusion in the study. Cases of encephalitis were defined based on criteria outlined by the International Encephalitis Consortium, with two categories, ‘probable/confirmed’ and ‘possible’. Other data collected included demographics, laboratory tests, underlying diseases and comorbidities, and deaths. We used mean (range) and absolute numbers (proportions) to report results, and compared quantitative and qualitative variables using Student’s t-test and Chi-squared, respectively.
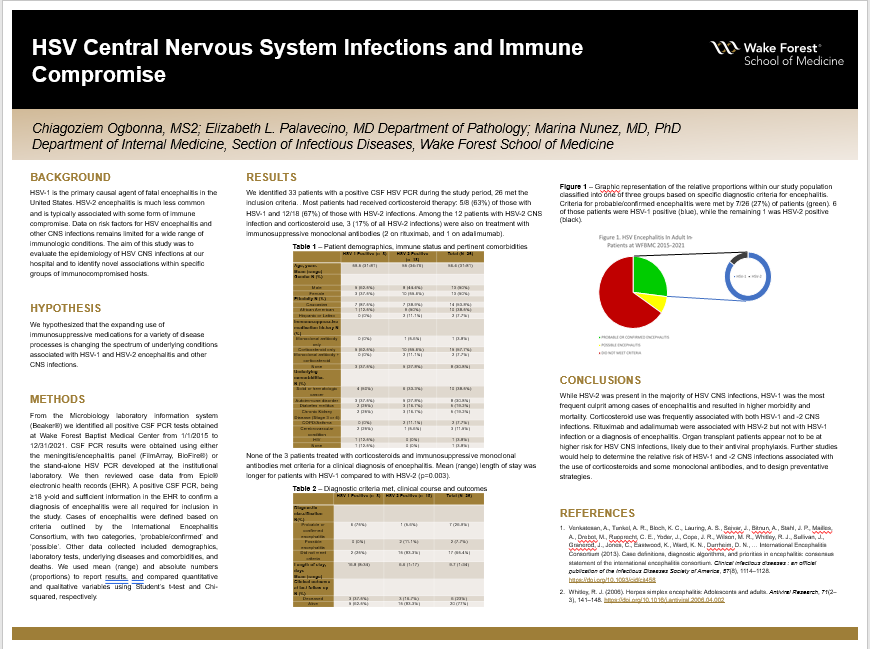
Results: Out of 33 patients with a positive CSF HSV PCR during the study period, 26 met the inclusion criteria. Their mean age was 56 years (range 31-81), 13 (50%) were male, and 14/26 (54%) Caucasian, 10/26 (38%) Black, and 2/26 (8%) Hispanic. HSV-2 predominated (18/26, 69%) over HSV-1 infections (8/26, 31%). Demographics were comparable for patients with HSV-1 and -2 infections. Ten out of the 26 (38%) had solid or hematologic cancer, 8 (31%) an autoimmune disorder, and 1 (4%) HIV infection, while 7 (27%) were not immunocompromised. None had a history of organ transplantation. Underlying conditions were comparable for patients with HSV-1 and -2 infections. Most patients had received corticosteroid therapy: 5/8 (63%) of those with HSV-1 and 12/18 (67%) of those with HSV-2 infections. Among the 12 patients with HSV-2 CNS infection and corticosteroid use, 3 (17% of all HSV-2 infections) were also on treatment with immunosuppressive monoclonal antibodies (2 on rituximab, and 1 on adalimumab). Criteria for probable/confirmed encephalitis were met by 6/8 (75%) patients with HSV-1 and by 1/18 (6%) with HSV-2, while possible encephalitis criteria were met by none with HSV-1 and 2/18 (11%) with HSV-2. The remaining 15 (83%) with HSV-2 did not meet the minimum criteria for either category. None of the 3 patients on treatment with corticosteroids and immunosuppressive monoclonal antibodies met the criteria for a clinical diagnosis of encephalitis. Mean (range) length of stay was significantly longer for patients with HSV-1 (17 (8-34) days) than for those with HSV-2 (7 (1-17) days); p=0.003. Death occurred in 3/8 (38%) of HSV-1 positive vs. 3/18 (17%) of HSV-2 positive subjects; p=.2.
Conclusions: While HSV-2 was present in the majority of HSV CNS infections, HSV-1 was the most frequent culprit among cases of encephalitis and resulted in higher morbidity and mortality. Corticosteroid use was frequently associated with both HSV-1 and -2 CNS infections. Rituximab and adalimumab were associated with HSV-2 but not with HSV-1 infection or a diagnosis of encephalitis. Organ transplant patients appear not to be at higher risk for HSV CNS infections, likely due to their antiviral prophylaxis. Further studies would help to determine the relative risk of HSV-1 and -2 CNS infections associated with the use of corticosteroids and some monoclonal antibodies, and to design preventative strategies.
Source of mentor’s funding or other support that funded this research: N/A
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy