 CLOSE SIDEBAR
CLOSE SIDEBAR
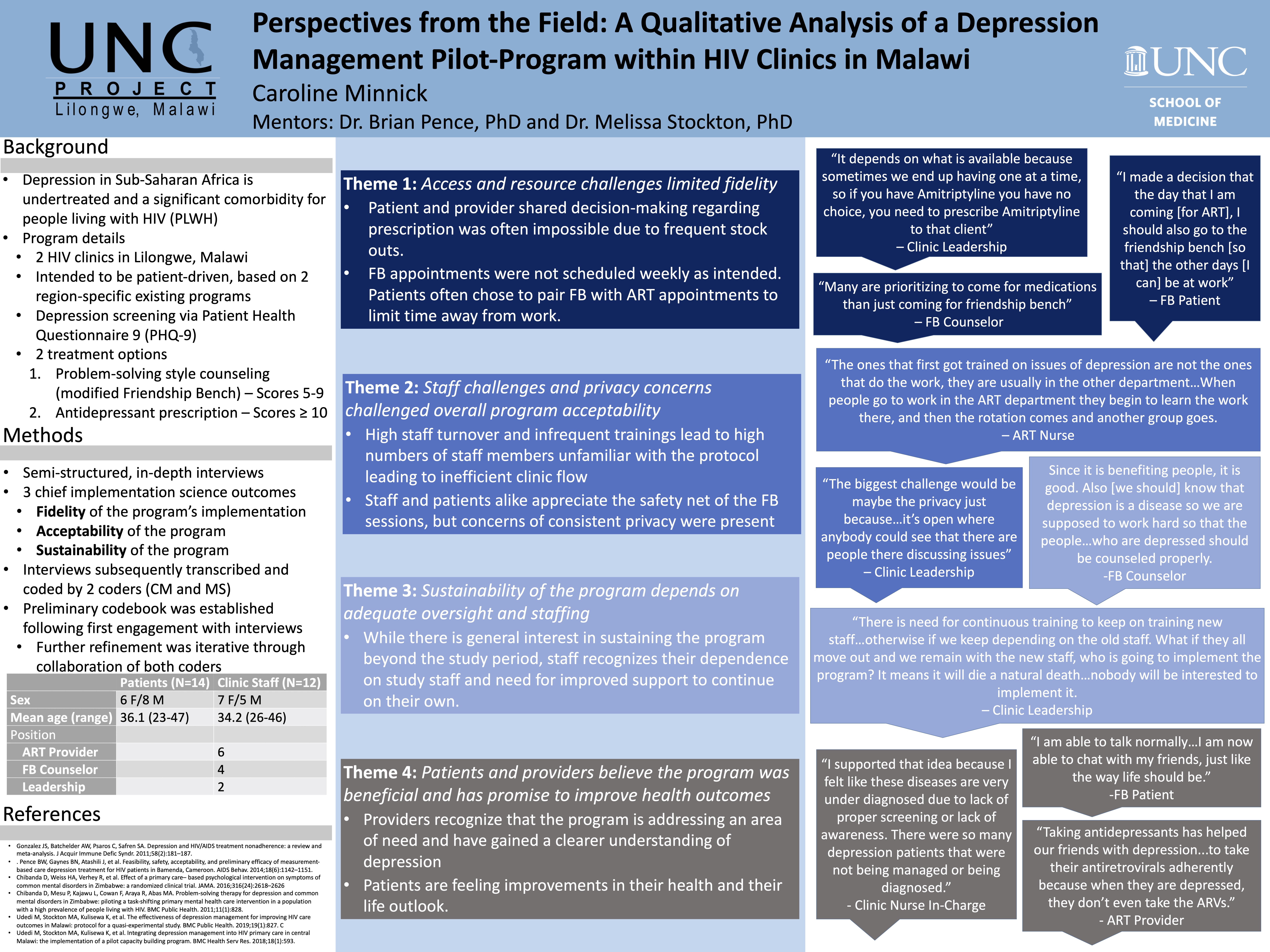
Perspectives from the Field: A Qualitative Analysis of a Depression Management Pilot- Program within HIV Clinics in Malawi
Caroline Minnick
Background: Depression is underdiagnosed, undertreated, and a significant comorbidity for people living with HIV (PLWH) in Sub-Saharan Africa (SSA). Though strides have been made to improve health outcomes for PLWH in SSA, depression remains a cause for unreliable adherence to HIV treatment and retention in care. To address this concern, the Malawi Ministry of Health (MOH) introduced a depression management program in 2 public HIV clinics in Lilongwe, Malawi, drawing from two evidence-based interventions tailored for SSA. Existing providers were trained to screen patients initiating HIV treatment for depression using the Patient Health Questionnaire-9 (PHQ-9) and refer depressed patients for appropriate intervention. The program utilized a measurement-based care (MBC) protocol for prescribing antidepressants (AD) for those with moderate to severe depression (PHQ-9 ≥ 10) and an adaptation of
the Friendship Bench (FB) problem-solving therapy for those with mild depression (PHQ-9 5-9).
Hypothesis: (1) The program will be implemented successfully with minimal deviations given its basis in 2 evidence-based interventions. (2) Both patients and providers will find that the program is beneficial, as it will reduce depressive symptoms and improve HIV care outcomes. (3) Utilization of existing clinic staff through a task-shifting protocol will allow the program to continue beyond the study period, given the infrequent and limited role study staff will play.
Methods: Our team designed and conducted semi-structured, comprehensive interviews with patients, providers, and leadership staff from both clinics. Interviewees shared their experiences receiving or providing care and with the pilot-program’s implementation. Interviews were recorded, transcribed, and coded to assess 3 key implementation science outcomes: fidelity, acceptability, and sustainability. Assessment of the interviews involved recognizing emerging themes, categorizing themes into one of our 3 key outcomes, and comparing these themes across interviews.
Results: While the program was acceptable to both patients and clinic staff, challenges of fidelity and sustainability clearly emerged. Interviews with providers and clinic leadership revealed protocol deviations related to AD selection, FB appointment scheduling, and follow-up PHQ-9 screening, often citing supply chain, time-constraints, and staffing challenges as causal. Many clinic staff shared concerns about the minimal training and high staff-turnover, both of which contributed to staffing challenges. FB counselors and patients alike appreciated the openness and intimacy of the FB but were concerned privacy was not always guaranteed. In general, patients found that the intervention positively impacted their lives. Finally, when addressing the sustainability of the program, most providers voiced concerns, highlighting their reliance upon study staff, limited bandwidth, and variable motivation in light of competing priorities. Moving forward, addressing program oversight, integration into existing clinic workflow, and improved and recurrent training may yield a more successful, sustainable initiative.
Conclusions: Though patients and providers reflected on the program’s intent and impact positively, continuation of the program beyond the given study period will be limited by personnel, resource, and leadership constraints. The addition of depression care to HIV clinics offers great promise in its ability to positively care for and improve outcomes of PHWH in SSA, but future programming should consider how to better interlace follow-up depression care with ART care to minimize additional time and resources needed from both patients and clinic staff.
Source of mentor’s funding or other support that funded this research: PEPFAR and USAID
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy