 CLOSE SIDEBAR
CLOSE SIDEBAR
Rapid Outpatient Follow-up Reduces Emergency Department Re-admission for Patients with Acute Chest Pain
Ryan Morgan
ABSTRACT
Background: Acute chest pain accounts for 7-10 million emergency department (ED) encounters each year. Less than 10% of chest pain patients who present to the ED are diagnosed with acute coronary syndrome (ACS), and nearly 1 in 10 patients return to the hospital within 7 days of discharge. The subsequent re-evaluation of these patients in the ED is inefficient, costly, and contributes to crowding.
Hypothesis: Patients who follow-up with a primary care physician or cardiologist within 15 days of ED discharge will have fewer 30-day ED re-admissions than patients who do not.
Methods: A retrospective cohort study was used to evaluate whether non-low-risk HEART Pathway patients in the Wake Forest Baptist Medical Center Emergency Department’s Clinical Decision Unit (ED CDU) had fewer 30-day ED re-admissions if they received rapid follow-up care than patients without follow-up. Non-low-risk adult patients (≥ 18 years old) with non-traumatic chest pain and no evidence of ST-elevation myocardial infarction who were being evaluated for ACS in the CDU from 3/1/2019-3/1/2020 were included. Non-low-risk was defined as patients with a HEAR score of 4 or more, a history of known coronary artery disease, or electrocardiogram findings concerning for possible ischemia. Descriptive statistics were performed. Fishers exact test was used to assess the association between 30-day readmissions and outpatient follow-up.
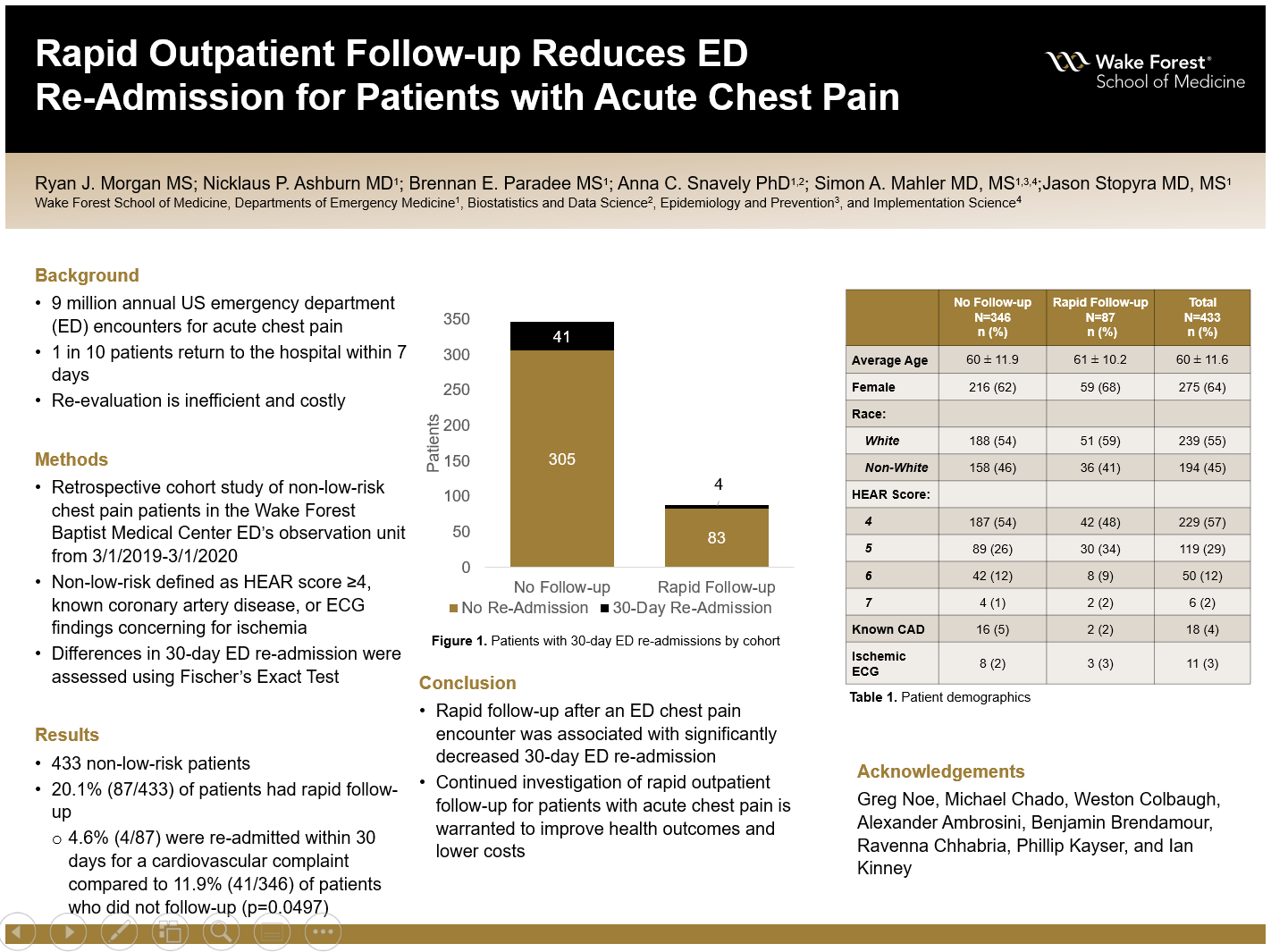
Results: There were 433 non-low-risk patients evaluated in the ED CDU. The cohort was 36% male, 55% white, and had a mean age of 60.2 years (SD ± 11.6). Among the 20.1% (87/433) of patients who followed-up with a provider within 15 days of their index ED visit, 4.6% (4/87) were re-admitted to the ED within 30 days for a cardiovascular complaint compared to 11.9% (41/346) of patients who did not follow-up (p=0.0497).
Conclusions: Rapid outpatient follow-up for non-low-risk chest pain patients who are discharged from the ED CDU was associated with decreased 15-day ED readmission.
Source of mentor’s funding or other support that funded this research: Atrium Health Wake Forest Baptist Department of Emergency Medicine
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy