 CLOSE SIDEBAR
CLOSE SIDEBAR
Clinical Characteristics Associated with Acute Pulmonary Emboli in SARS-CoV-2 Positive Patients in the Emergency Department Setting
Kevin Alexander Soltany
Background: There is growing research documenting the incidence of acute pulmonary embolism (PE) in hospitalized patients with COVID-19, yet few published studies investigate the association between SARS-CoV-2 infection and acute PE upon initial presentation to the emergency department (ED). This study aims to compare the diagnostic yield of CTPA for PE in COVID-19 ED patients, review traditional ED algorithms for suspected PE, and examine how clinical characteristics can be utilized to improve CTPA yield for PE.
Hypothesis: (1) The diagnostic yield of CTPA for evaluation of PE in the setting of COVID-19 patients presenting to the ED will be significantly higher than that of a similar cohort of ED patients with suspicion of PE one year prior. (2) Patients in the study cohort with a diagnosis of PE on CTPA will have significantly higher D-dimer levels, average ages, BMIs, and heart rates when compared to those with a negative CTPA study.
Methods: This is a multicenter retrospective chart review of pediatric and adult patients who arrived to any of the five Wake Forest Baptist Health EDs from 3/17/2020-1/31/2021. The study cohort included patients with a positive COVID-19 test or a COVID-related diagnosis and a CTPA ordered while in the ED. The overall CTPA yield for PE within this study cohort was calculated and compared to that of a control cohort of patients who presented to the ED during a period one year prior to the study cohort and had a CTPA study ordered. We compared demographics and clinical characteristics of patients within the study cohort.
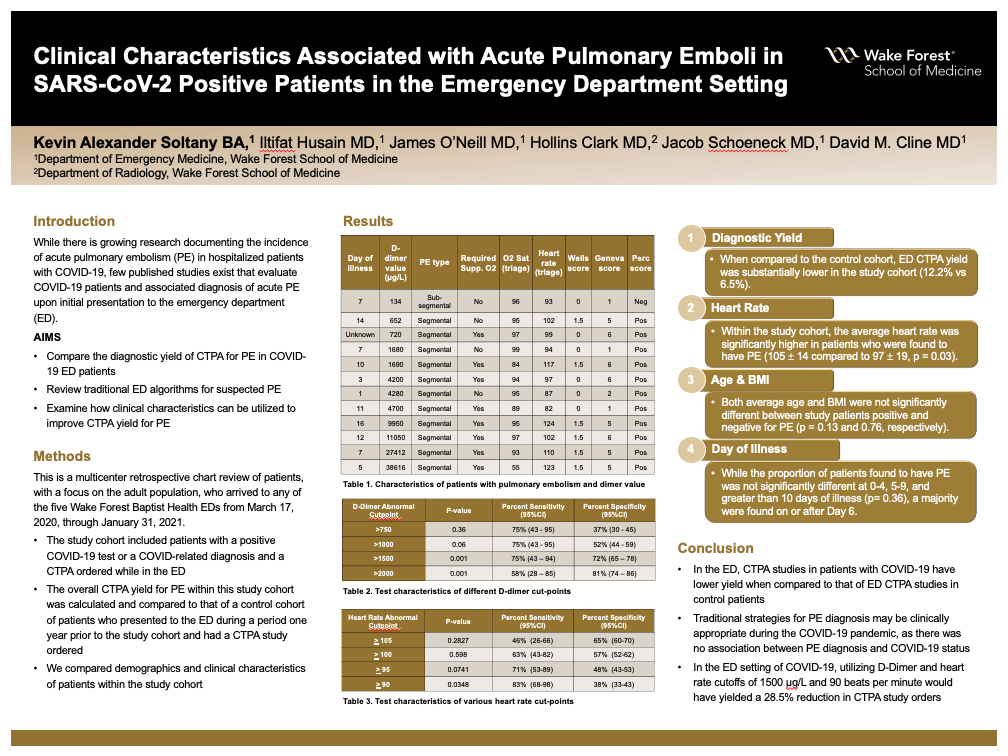
Results: 425 patients were identified by discharge diagnosis as having undergone evaluation for PE in the setting of suspected COVID-19 infection during the study period. Of this cohort, 370 patients (87.1%) tested positive for SARS-CoV-2 infection and underwent CTPA for suspected PE. 23 patients (6.5%) were ultimately found to have a PE on CTPA. Within the study cohort, the average heart rate was significantly higher in patients who were found to have PE (105 ± 14 compared to 97 ± 19, p = 0.03), while both average age and BMI were not significantly different (p = 0.13 and 0.76, respectively). Of those who underwent D-dimer testing, abnormal D-dimer had a sensitivity of 86% (CI 57-89%) and specificity of 14% (CI 9-19%) for diagnosis of PE. No patients with both a D-Dimer less than 1500 μg/L and a heart rate less than 90 beats per minute were found to have PE. When compared to the control cohort, ED CTPA yield was substantially lower in the study cohort (12.2% vs 6.5%).
Conclusions: In the ED, CTPA studies in patients with COVID-19 have lower yield when compared to that of ED CTPA studies in control patients. Traditional strategies for PE diagnosis may be clinically appropriate during the COVID-19 pandemic, as there was no association between PE diagnosis and COVID-19 status. In the setting of COVID-19, utilizing D-Dimer and heart rate cutoffs of 1500 μg/L and 90 beats per minute would have yielded a 28.5% reduction in CTPA study orders.
Powered by Acadiate
© 2011-2024, Acadiate Inc. or its affiliates · Privacy